You might also like
- The Borax ConspiracyDocument14 pagesThe Borax ConspiracyMiroslav Ilic94% (48)
- Attachment Part Two - Developing SecurityDocument8 pagesAttachment Part Two - Developing Securitywonder_full77No ratings yet
- Effective Leadership and Management in NursingDocument2 pagesEffective Leadership and Management in NursingRey VegaNo ratings yet
- American Board of Family Medicine: TTT SAMPLE TTTDocument72 pagesAmerican Board of Family Medicine: TTT SAMPLE TTTSalah Elbadawy100% (1)
- Heart Failure and CAD Case StudyDocument38 pagesHeart Failure and CAD Case StudyAbno NavarreteNo ratings yet
- Melanoma CaseDocument4 pagesMelanoma CaseDinarkram Rabreca EculNo ratings yet
- Anna Dabu M.D. University of Western Ontario June 2009Document18 pagesAnna Dabu M.D. University of Western Ontario June 2009Anna DabuNo ratings yet
- Anatomy and Pathophysiology of ProstrateDocument44 pagesAnatomy and Pathophysiology of Prostraterajan kumar100% (3)
- Current Trends in Management of CholedocholithiasisDocument35 pagesCurrent Trends in Management of Choledocholithiasisrajan kumar100% (6)
- Drugs in SportDocument180 pagesDrugs in Sportaermal89100% (1)
- Drug Studies (Common Drugs Used in The Delivery Room)Document6 pagesDrug Studies (Common Drugs Used in The Delivery Room)Elle100% (2)
- Aerobic Exercise: Marching in PlaceDocument4 pagesAerobic Exercise: Marching in Placenemica tamayaoNo ratings yet
- Pharm RemediationDocument5 pagesPharm RemediationAudrey WatsonNo ratings yet
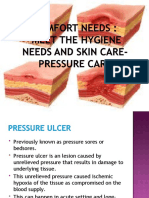
- What Is Pressure Ulcer?: Signs and SymptomsDocument6 pagesWhat Is Pressure Ulcer?: Signs and Symptomsshenecajean carajayNo ratings yet
- Pressure Ulcer CareDocument26 pagesPressure Ulcer CarekurapotaNo ratings yet
- Preventing Patient FallsDocument14 pagesPreventing Patient FallsyplianNo ratings yet
- Pressure UlcerDocument22 pagesPressure UlcerMakanjuola Osuolale John100% (2)
- Bed Sore 48Document45 pagesBed Sore 48Sedaka DonaldsonNo ratings yet
- 2 - Pressure UlcersDocument64 pages2 - Pressure Ulcerscharity kalinowsky100% (5)
- Early AdulthoodDocument1 pageEarly AdulthoodCherry BobierNo ratings yet
- NCP CHF Er SettingDocument9 pagesNCP CHF Er SettingroseasNo ratings yet
- Pressure SoresDocument20 pagesPressure SoresRupika Sodhi100% (1)
- Pressure UlcerDocument59 pagesPressure UlcerCresco Real EstateNo ratings yet
- Blood Transfusion ESSAY 1 1Document3 pagesBlood Transfusion ESSAY 1 1Ednilson Domingos0% (1)
- Post Op Assessment SurgeryDocument20 pagesPost Op Assessment SurgeryAbdullah MatarNo ratings yet
- Nursing Trends and IssuesDocument20 pagesNursing Trends and IssuesSri EndriyaniNo ratings yet
- The Management of Pressure Ulcers in Primary and Secondary Care PDFDocument464 pagesThe Management of Pressure Ulcers in Primary and Secondary Care PDFDragos-Ronald RugescuNo ratings yet
- Dka Management of Dka in Adults March 20101Document24 pagesDka Management of Dka in Adults March 20101djizhieeNo ratings yet
- Top 10 Care Essentials in Ventilated PtsDocument3 pagesTop 10 Care Essentials in Ventilated PtsAdel HamadaNo ratings yet
- Orientation Booklet For Emergency DepartmentDocument10 pagesOrientation Booklet For Emergency Departmentshahidchaudhary100% (1)
- Delirium: Acute Confusion in The Elderly: Donald R. Noll DO FACOIDocument53 pagesDelirium: Acute Confusion in The Elderly: Donald R. Noll DO FACOIHema Laughsalot100% (2)
- Respiratory Assessment FindingsDocument197 pagesRespiratory Assessment Findingsannatw100% (2)
- Ethics - Nursing Shortage IssueDocument7 pagesEthics - Nursing Shortage Issueapi-355702962No ratings yet
- Leadership Nursing and Patient SafetyDocument172 pagesLeadership Nursing and Patient SafetyRolena Johnette B. PiñeroNo ratings yet
- Describing WoundsDocument4 pagesDescribing WoundsDidikPrasetyoSuliNo ratings yet
- Disseminated Intravascular CoagulationDocument7 pagesDisseminated Intravascular CoagulationGennely Dolino Schwartz100% (1)
- KNH 413 Dka Case Study 2Document15 pagesKNH 413 Dka Case Study 2api-301897220100% (1)
- Study On Pressure UlcerDocument219 pagesStudy On Pressure UlcerThein Ko Oo100% (1)
- PolypharmacyDocument4 pagesPolypharmacyJeffrey Tan100% (1)
- Medical Assistance in Dying NewDocument4 pagesMedical Assistance in Dying NewNarinder S.No ratings yet
- Modified Braden Q ScaleDocument8 pagesModified Braden Q Scaleapi-122501165No ratings yet
- Pressure Ulcer Prevention and Managment PolicyDocument32 pagesPressure Ulcer Prevention and Managment PolicybudimanNo ratings yet
- Hypoglycemia: Presented by Farse GhabayenDocument11 pagesHypoglycemia: Presented by Farse GhabayenFares G. Ghabayen100% (2)
- SC IM InjectionDocument16 pagesSC IM InjectionMuhammad AbukhaterNo ratings yet
- Effective Communication in NursingDocument19 pagesEffective Communication in NursingChamCham AquinoNo ratings yet
- Nursing - Burn InjuryDocument39 pagesNursing - Burn Injuryamaracha2003No ratings yet
- Wound Infection Best PracticeDocument12 pagesWound Infection Best PracticeAnonymous 1nMTZWmzNo ratings yet
- Pressure Ulcers and Wounds: by Monica Warhaftig, D.O. Assistant Professor of Geriatrics N.S.UDocument64 pagesPressure Ulcers and Wounds: by Monica Warhaftig, D.O. Assistant Professor of Geriatrics N.S.UEvaNo ratings yet
- Staffing Nursing Management ReportDocument54 pagesStaffing Nursing Management ReportTin MagbanuaNo ratings yet
- The Role of Nurse Practitioners in Care Coordination and TransitionDocument10 pagesThe Role of Nurse Practitioners in Care Coordination and Transitionapi-312364579No ratings yet
- Pressure Ulcers and Hydrocolloids Made EasyDocument6 pagesPressure Ulcers and Hydrocolloids Made EasyJefferson AlexandreNo ratings yet
- Preoperative and Post Liver Transplant Nursing Care Plan, Nursing ProcessDocument2 pagesPreoperative and Post Liver Transplant Nursing Care Plan, Nursing ProcessOctoober100% (3)
- Jordan University of Science and Technology Faculty of NursingDocument14 pagesJordan University of Science and Technology Faculty of NursingAshraf Ali Smadi92% (13)
- Nursing Theories Goal AttainmentDocument9 pagesNursing Theories Goal AttainmentAmbili AneeshaNo ratings yet
- Nursing ShortageDocument10 pagesNursing Shortageالأغا محمد زكارنةNo ratings yet
- Clinical Nursing JudgmentDocument5 pagesClinical Nursing Judgmentapi-546730313No ratings yet
- Clinical Decision MakingDocument8 pagesClinical Decision Makingapi-400245000100% (1)
- Hourly Nursing Rounding & Call Bell ResponseDocument38 pagesHourly Nursing Rounding & Call Bell ResponseFSN Admin100% (2)
- Chapter - 001 Health Promotion in Middle-Aged AdultsDocument10 pagesChapter - 001 Health Promotion in Middle-Aged AdultsTrixie AlvarezNo ratings yet
- Pressure Ulcers: Problems and ChallengesDocument23 pagesPressure Ulcers: Problems and Challengesedi edong100% (1)
- Prevention of Surgical Site InfectionDocument10 pagesPrevention of Surgical Site InfectionValiant Baybay100% (1)
- Management of Dengue Fever in Children PDFDocument41 pagesManagement of Dengue Fever in Children PDFnakalnakal2015No ratings yet
- Fall PreventionDocument24 pagesFall Preventionlittleshortgurl100% (1)
- University of Perpetual Help System DALTA College of Nursing Batch 2010 2011Document5 pagesUniversity of Perpetual Help System DALTA College of Nursing Batch 2010 2011Shishi M. Pinlac100% (1)
- Abcde ApproachDocument3 pagesAbcde ApproachMaria Isabel Medina MesaNo ratings yet
- Wound Classification: Presented by Dr. Karen Zulkowski, D.N.S., RN Montana State UniversityDocument41 pagesWound Classification: Presented by Dr. Karen Zulkowski, D.N.S., RN Montana State UniversityDevasyaNo ratings yet
- A Simple Guide to Hypertension and Heart DiseasesFrom EverandA Simple Guide to Hypertension and Heart DiseasesRating: 5 out of 5 stars5/5 (1)
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Current Role of Surgery in The Management of Peptic UlceDocument19 pagesCurrent Role of Surgery in The Management of Peptic Ulcerajan kumarNo ratings yet
- Carcinoma Gall BladderDocument25 pagesCarcinoma Gall Bladderrajan kumarNo ratings yet
- Pathophysiology of TBI 97Document51 pagesPathophysiology of TBI 97rajan kumarNo ratings yet
- Adrenal and PheochromocytomaDocument86 pagesAdrenal and Pheochromocytomarajan kumar100% (1)
- Head Injury ManagementDocument11 pagesHead Injury Managementrajan kumar100% (1)
- Abdominal Tbpresentation Diagnosis and Treatment NewDocument36 pagesAbdominal Tbpresentation Diagnosis and Treatment Newrajan kumar100% (3)
- Principles and Practice of GI EndosDocument101 pagesPrinciples and Practice of GI Endosrajan kumar90% (21)
- Prospects of Breast Reconstruction in LABCDocument22 pagesProspects of Breast Reconstruction in LABCrajan kumarNo ratings yet
- MeningomyeloceleDocument34 pagesMeningomyelocelerajan kumarNo ratings yet
- Management of The Hydrocephalus and OutcomeDocument24 pagesManagement of The Hydrocephalus and Outcomerajan kumar100% (1)
- HydrocephalusDocument33 pagesHydrocephalusrajan kumar100% (2)
- Ca PenisDocument25 pagesCa Penisrajan kumar100% (2)
- Evaluation of Factors Influencing Morbidity and Mortality in Cases of Oesophageal Atresia And/or Tracheo-Oesophageal Fistula RepairDocument26 pagesEvaluation of Factors Influencing Morbidity and Mortality in Cases of Oesophageal Atresia And/or Tracheo-Oesophageal Fistula Repairrajan kumarNo ratings yet
- Principles of CT Scan AbdomenDocument101 pagesPrinciples of CT Scan Abdomenrajan kumar100% (16)
- Work Up of Gynecomastia (Slides)Document22 pagesWork Up of Gynecomastia (Slides)rajan kumar67% (3)
- Graves' Disease & PregnancyDocument19 pagesGraves' Disease & Pregnancyrajan kumar100% (1)
- Mechanical Ventilation SeminarDocument82 pagesMechanical Ventilation Seminarrajan kumar90% (21)
- Liver TransplantationDocument22 pagesLiver Transplantationrajan kumar100% (6)
- Approach To Thyroid NoduleDocument33 pagesApproach To Thyroid Nodulerajan kumar100% (5)
- Blood ProductDocument35 pagesBlood Productrajan kumar100% (3)
- Complications of Laparoscopic SurgeriesDocument40 pagesComplications of Laparoscopic Surgeriesrajan kumar100% (10)
- Tracheo-Oesophageal FistulaDocument19 pagesTracheo-Oesophageal Fistularajan kumar100% (3)
- Buergers DiseaseDocument30 pagesBuergers Diseaserajan kumar100% (9)
- Jurnal Harry StackDocument4 pagesJurnal Harry StackmikeNo ratings yet
- Quackery Mapeh 10Document23 pagesQuackery Mapeh 10CASSEY ANNE LARA100% (2)
- Cryolipolysis Body Slimming Machine Nbw-c132-User ManualDocument22 pagesCryolipolysis Body Slimming Machine Nbw-c132-User ManualRodrigo Centurion100% (1)
- Presented By: Christopher H. Wise, PT, DPT, MS, OCS, FAAOMPT, MTC, ATCDocument1 pagePresented By: Christopher H. Wise, PT, DPT, MS, OCS, FAAOMPT, MTC, ATCemilNo ratings yet
- 120 1 312 1 10 20170109Document4 pages120 1 312 1 10 20170109Riza TamaNo ratings yet
- FJLGKKJFBVN, KhkdsljhlkxcidhlisxhfkjdbfhlkjdsbhflkudshljxzhbDocument931 pagesFJLGKKJFBVN, KhkdsljhlkxcidhlisxhfkjdbfhlkjdsbhflkudshljxzhbTalal HajNo ratings yet
- LovenoxDocument1 pageLovenoxKatie McPeek100% (2)
- Ccu PSG en DysphagiaDocument52 pagesCcu PSG en DysphagiaTni JolieNo ratings yet
- Non Steroidal Anti Inflammatory DrugDocument21 pagesNon Steroidal Anti Inflammatory DrugRanganath NagarajNo ratings yet
- Clinical Skills: Explaining Malaria To A Patient: WWW - Osce-Aid - Co.ukDocument2 pagesClinical Skills: Explaining Malaria To A Patient: WWW - Osce-Aid - Co.ukRisfandi Ahmad TaskuraNo ratings yet
- Shendi Obs OsceDocument35 pagesShendi Obs OsceYassin Jamal67% (3)
- Correctional NewsDocument48 pagesCorrectional NewsAndrewNo ratings yet
- Acute Decompensated Heart FailureDocument31 pagesAcute Decompensated Heart Failure568563No ratings yet
- Kidney TransplantDocument1 pageKidney Transplantsunilk09No ratings yet
- Pneumothorax: DR G.B.L Samarasekera Consultant Respiratory Physician DGH - GampahaDocument50 pagesPneumothorax: DR G.B.L Samarasekera Consultant Respiratory Physician DGH - GampahappgpcsNo ratings yet
- Hall - Harrigan - Nonverbal Behavior in Clinician-Patient InteractionDocument17 pagesHall - Harrigan - Nonverbal Behavior in Clinician-Patient InteractionGeorge BaciuNo ratings yet
- What Causes Cataract?Document3 pagesWhat Causes Cataract?Eye spacialistNo ratings yet
- Comparison of Pregabalin With PramipexoleDocument49 pagesComparison of Pregabalin With PramipexoleFrans JobethNo ratings yet
- Asthma AlgorithmDocument13 pagesAsthma Algorithmgamecockusc1992No ratings yet
- Case ReportDocument50 pagesCase ReportTajul AnshorNo ratings yet
- Neonatal Ventilator Vent Set-Up CheatsheetDocument1 pageNeonatal Ventilator Vent Set-Up CheatsheetRick Frea50% (2)
- Bracket PositionDocument10 pagesBracket PositionBarsha ThapaNo ratings yet
- Sociology Final ProjectDocument16 pagesSociology Final Projectabt09No ratings yet