You might also like
- Improving The Quality of Care in An Acute Care Facility Through RDocument88 pagesImproving The Quality of Care in An Acute Care Facility Through RNor-aine Salazar AccoyNo ratings yet
- Counselling, Breaking Bad NewsDocument26 pagesCounselling, Breaking Bad NewsArief NorddinNo ratings yet
- An Integrative Literature Review On Post Organ Transplant Mortality Due To Renal Failure: Causes and Nursing CareDocument18 pagesAn Integrative Literature Review On Post Organ Transplant Mortality Due To Renal Failure: Causes and Nursing CarePATRICK OTIATONo ratings yet
- Ethical Dilemmas in Nursing PDFDocument5 pagesEthical Dilemmas in Nursing PDFtitiNo ratings yet
- WP Leadership StandardsDocument44 pagesWP Leadership StandardsIfrah Harun100% (1)
- Law of Delict PPPDocument22 pagesLaw of Delict PPPPragash Maheswaran100% (3)
- AOA Survival Guide To The 2nd YearDocument18 pagesAOA Survival Guide To The 2nd Yearmediquest100% (1)
- Corruption and Abuse of Office by PublicDocument13 pagesCorruption and Abuse of Office by PublicAbubakar UmarNo ratings yet
- US Vs Ah Chong, L-5272, March 19, 1910, 15 Phil. 488 (1910)Document7 pagesUS Vs Ah Chong, L-5272, March 19, 1910, 15 Phil. 488 (1910)Maria50% (2)
- Falls Among Older AdultsDocument59 pagesFalls Among Older AdultsShahrul Hafiz100% (1)
- Revision Notes Criminal LawDocument7 pagesRevision Notes Criminal Lawwatever100% (1)
- + Rhodes - A Systematic Approach To Clinical Moral Reasoning (Clinical Ethics 2007)Document6 pages+ Rhodes - A Systematic Approach To Clinical Moral Reasoning (Clinical Ethics 2007)Mercea AlexNo ratings yet
- Falls in Older PeopleDocument18 pagesFalls in Older PeoplePabloIgLopezNo ratings yet
- Japan's Government Social Policy On Management of Aging SocietyDocument7 pagesJapan's Government Social Policy On Management of Aging SocietyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- EBMDocument636 pagesEBMDaniel SalaNo ratings yet
- LeprosyDocument16 pagesLeprosyPriscilla Sund Nguyen100% (2)
- Advanced Practice in Nursing and the Allied Health ProfessionsFrom EverandAdvanced Practice in Nursing and the Allied Health ProfessionsPaula McGeeNo ratings yet
- Platon Notes - Obligations & Contracts (Gonzales)Document98 pagesPlaton Notes - Obligations & Contracts (Gonzales)Gracee Ramat0% (1)
- Multidisciplinary Team and Pharmacists Role in That TeamDocument5 pagesMultidisciplinary Team and Pharmacists Role in That TeamTimothy OgomaNo ratings yet
- Pros Sagssago Notes in Criminal Law 2017 EditionDocument316 pagesPros Sagssago Notes in Criminal Law 2017 EditionLEIGH100% (1)
- Health Systems Strengthening - The University of MelbourneDocument14 pagesHealth Systems Strengthening - The University of MelbourneEstefanía MariñoNo ratings yet
- (Full) Concept of Quasi-Delict ElementsDocument77 pages(Full) Concept of Quasi-Delict ElementsSasha BrausNo ratings yet
- Reflective Writing b8ll100Document22 pagesReflective Writing b8ll100Nurin HadNo ratings yet
- Rodriguez V Ponferrada DigestDocument1 pageRodriguez V Ponferrada DigestDrew Dalapu100% (1)
- Change InitiativeDocument7 pagesChange InitiativeWajiha ShaikhNo ratings yet
- 1 SyringomyeliaDocument26 pages1 SyringomyeliaYosafat Ate100% (1)
- Professional Accountability in NursingDocument4 pagesProfessional Accountability in NursingJohn N MwangiNo ratings yet
- Creating the Health Care Team of the Future: The Toronto Model for Interprofessional Education and PracticeFrom EverandCreating the Health Care Team of the Future: The Toronto Model for Interprofessional Education and PracticeNo ratings yet
- Ethical Issues in Palliative CareDocument18 pagesEthical Issues in Palliative CareDinesh DNo ratings yet
- Alcoholic NeuropathyDocument4 pagesAlcoholic Neuropathyhis.thunder122100% (1)
- Module Guide For Palliative Care AssessmentDocument83 pagesModule Guide For Palliative Care AssessmentAnd ReiNo ratings yet
- Spirituality in Healthcare: Perspectives for Innovative PracticeFrom EverandSpirituality in Healthcare: Perspectives for Innovative PracticeNo ratings yet
- Dialysis Without Fear PDFDocument273 pagesDialysis Without Fear PDFandrada14No ratings yet
- The WHO Health Promotion Glossary PDFDocument17 pagesThe WHO Health Promotion Glossary PDFfirda FibrilaNo ratings yet
- The Child With Spina Bifida PDFDocument365 pagesThe Child With Spina Bifida PDFAna H.No ratings yet
- Ppta Standards of PracticeDocument3 pagesPpta Standards of PracticeChaddyBabeNo ratings yet
- Tools Iowa Ebnp-1 PDFDocument10 pagesTools Iowa Ebnp-1 PDFNovita Surya100% (1)
- Thesis (Noridja's Group)Document31 pagesThesis (Noridja's Group)DenMarkSolivenMacniNo ratings yet
- Organ DonationDocument9 pagesOrgan DonationAravindan Sundar100% (1)
- 3806NRS Nursing Assignment HelpDocument5 pages3806NRS Nursing Assignment HelpMarry WillsonNo ratings yet
- Introduction To Nursing Research Part 1Document22 pagesIntroduction To Nursing Research Part 1Ciedelle Honey Lou DimaligNo ratings yet
- Psychological ChangesDocument36 pagesPsychological ChangesAndrei La MadridNo ratings yet
- 3melnyk Ebp Asking Clinical QuestionDocument4 pages3melnyk Ebp Asking Clinical Questionapi-272725467No ratings yet
- Providing Culturally Appropriate Care: A Literature ReviewDocument9 pagesProviding Culturally Appropriate Care: A Literature ReviewLynette Pearce100% (1)
- Knowledge, Attitude and Practices (KAP) Studies Conducted Amongst Medical Students of IndiaDocument6 pagesKnowledge, Attitude and Practices (KAP) Studies Conducted Amongst Medical Students of IndiaAnonymous x8fY69CrnNo ratings yet
- Department of Health Departmental Report 2008Document253 pagesDepartment of Health Departmental Report 2008Bren-RNo ratings yet
- Oedojo Soedirham) : Department of Health Promotion and Behavioral SciencesDocument59 pagesOedojo Soedirham) : Department of Health Promotion and Behavioral SciencesAshri Nur IstiqomahNo ratings yet
- Original EssayDocument3 pagesOriginal EssayAj AquinoNo ratings yet
- Islam and Palliative CareDocument16 pagesIslam and Palliative CareShirakawa AlmiraNo ratings yet
- Time To Learn. Understanding Patient Centered CareDocument7 pagesTime To Learn. Understanding Patient Centered CareAden DhenNo ratings yet
- 20191212002111week 2 Assignment Nursing ResearchDocument2 pages20191212002111week 2 Assignment Nursing ResearchkelvinNo ratings yet
- Postop Physical Therapy in Orthopedic PatientsDocument1 pagePostop Physical Therapy in Orthopedic PatientsnvvharikrishnaNo ratings yet
- Recognising and Defining Clinical Nurse LeadersDocument4 pagesRecognising and Defining Clinical Nurse LeadersSholihatul AmaliyaNo ratings yet
- Rehabilitation Grand Rounds NURS 441 - Clinical Management of Recovery Purpose of AssignmentDocument3 pagesRehabilitation Grand Rounds NURS 441 - Clinical Management of Recovery Purpose of Assignmentapi-348670719No ratings yet
- Newborn AssessmentDocument4 pagesNewborn Assessmentapi-400252098No ratings yet
- Unit 29 Health PromotionDocument4 pagesUnit 29 Health Promotionchandni0810100% (1)
- Evidence Based PracticesDocument5 pagesEvidence Based Practicesapi-527787868No ratings yet
- Impact of Fall Prevention Program Upon Elderly Behavior Related Knowledge at Governmental Elderly Care Homes in Baghdad CityDocument7 pagesImpact of Fall Prevention Program Upon Elderly Behavior Related Knowledge at Governmental Elderly Care Homes in Baghdad CityIOSRjournalNo ratings yet
- Ebp Formative Synthesis PaperDocument9 pagesEbp Formative Synthesis Paperapi-404415990No ratings yet
- Refining A Self-Assessment of Informatics Competency Scale Using Mokken Scaling AnalysisDocument9 pagesRefining A Self-Assessment of Informatics Competency Scale Using Mokken Scaling AnalysisTenIs ForMeNo ratings yet
- Nursing PhilosDocument8 pagesNursing Philosapi-527531404No ratings yet
- Piel Et Al - Understanding The Global Dimensions of Health (2005)Document303 pagesPiel Et Al - Understanding The Global Dimensions of Health (2005)Jaime Fernández-Aguirrebengoa100% (1)
- Stroke Canadian2010Document247 pagesStroke Canadian2010Dewi LuhNo ratings yet
- ACC1162 OEP To Prevent Falls in Older Adults - Jul07Document72 pagesACC1162 OEP To Prevent Falls in Older Adults - Jul07moliceiraNo ratings yet
- Use of Sedation in Palliative CareDocument13 pagesUse of Sedation in Palliative Careuriel_rojas_41No ratings yet
- Simulation & Gaming at NIDocument3 pagesSimulation & Gaming at NIFrancis ObmergaNo ratings yet
- MPU3313 MPU2313 Topic 6Document26 pagesMPU3313 MPU2313 Topic 6CheAzahariCheAhmad100% (1)
- PL - Platinum 01 - 07 - 2021Document52 pagesPL - Platinum 01 - 07 - 2021Nugraha Dwi Ananta RNNo ratings yet
- HP 2000 Inventec 6050A2498701-MB-A02 AMD PDFDocument45 pagesHP 2000 Inventec 6050A2498701-MB-A02 AMD PDFyenny naveaNo ratings yet
- Lenovo NM-A471 PDFDocument59 pagesLenovo NM-A471 PDFRat Noe0% (1)
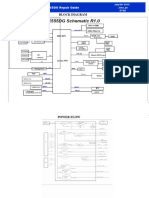
- Block Diagram: X555DG Repair GuideDocument5 pagesBlock Diagram: X555DG Repair GuideNugraha Dwi Ananta RN100% (1)
- Compal Confidential: P1VE6 LA7071P Schematics DocumentDocument37 pagesCompal Confidential: P1VE6 LA7071P Schematics DocumentChristiam OrtegaNo ratings yet
- Biostar H81MDV3 SpecDocument8 pagesBiostar H81MDV3 SpecNugraha Dwi Ananta RNNo ratings yet
- Rock S A0001118475 1Document49 pagesRock S A0001118475 1abg tuaNo ratings yet
- Sony MBX-208 - Quanta SY2 - MB - 0409cDocument36 pagesSony MBX-208 - Quanta SY2 - MB - 0409cNugraha Dwi Ananta RNNo ratings yet
- Toms River Regional School District Athletic Waiver and Release of Liability Form Related To COVID-19Document4 pagesToms River Regional School District Athletic Waiver and Release of Liability Form Related To COVID-19Asbury Park PressNo ratings yet
- Dela Llano Vs BiongDocument6 pagesDela Llano Vs BiongWhatever123456789No ratings yet
- Barredo v. GarciaDocument2 pagesBarredo v. GarciaGela Bea BarriosNo ratings yet
- PTE Academic Online Test Taker Handbook - May 2022Document28 pagesPTE Academic Online Test Taker Handbook - May 2022Tommy Linny H.No ratings yet
- TortsDocument2 pagesTortsGalanza FaiNo ratings yet
- Casupanan Vs LaroyaDocument8 pagesCasupanan Vs LaroyaKristine KristineeeNo ratings yet
- CLJ 3 Week 5-10Document13 pagesCLJ 3 Week 5-10Gierlie Viel MogolNo ratings yet
- United States v. Leslie Roberts, 978 F.2d 17, 1st Cir. (1992)Document12 pagesUnited States v. Leslie Roberts, 978 F.2d 17, 1st Cir. (1992)Scribd Government DocsNo ratings yet
- Crim Fact ScenarioDocument2 pagesCrim Fact ScenarioGouri DasNo ratings yet
- Draft IRR RA 10606 - Natl Health Ins Act 2013Document103 pagesDraft IRR RA 10606 - Natl Health Ins Act 2013roy rubaNo ratings yet
- 021 Samson v. Restrivera PDFDocument3 pages021 Samson v. Restrivera PDFDan Del RosarioNo ratings yet
- Package Description: Manila Ocean Park Attractions PassDocument8 pagesPackage Description: Manila Ocean Park Attractions PassRenato OrosaNo ratings yet
- LEGMED CaseDocument16 pagesLEGMED CaseGabriel Jhick SaliwanNo ratings yet
- Far East Bank vs. CADocument5 pagesFar East Bank vs. CAMan HernandoNo ratings yet
- TORT Midterm ExamDocument6 pagesTORT Midterm ExamJenieNo ratings yet
- Cinco Vs CanonoyDocument5 pagesCinco Vs CanonoyChristine ErnoNo ratings yet
- Medical NegligenceDocument29 pagesMedical NegligenceVishwajeet GandhiNo ratings yet
- Nature and Scope of Law of Torts - Author - Lakshmi SomanathanDocument5 pagesNature and Scope of Law of Torts - Author - Lakshmi SomanathanJasmine Singh100% (1)
- GEAC Self Declaration FormDocument3 pagesGEAC Self Declaration FormJenny CroweNo ratings yet
- 20ba086 GPCL PROJECT 2022Document16 pages20ba086 GPCL PROJECT 2022sayed abdul jamayNo ratings yet
- Filamer Vs Iac (LABOR LAW)Document5 pagesFilamer Vs Iac (LABOR LAW)Athena Venice MercadoNo ratings yet
- Draft Articles On The Responsibility of International Organizations (2011)Document16 pagesDraft Articles On The Responsibility of International Organizations (2011)ebrtzNo ratings yet