You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nikolas Rose - Neurochemical Selves - Society, Nov/Dec 2003Document14 pagesNikolas Rose - Neurochemical Selves - Society, Nov/Dec 2003kod65redNo ratings yet
- Farmacoterapia para TOC ResistenteDocument3 pagesFarmacoterapia para TOC ResistenteSusana Pérez ReyesNo ratings yet
- 966baf PDFDocument86 pages966baf PDFkaw gd100% (2)
- 2ND and 3RD Drug StudyDocument16 pages2ND and 3RD Drug Study황춘히No ratings yet
- Panic Disorder Treatment GuidelinesDocument3 pagesPanic Disorder Treatment Guidelinesputri weniNo ratings yet
- I. See Also: AdvertisementDocument35 pagesI. See Also: AdvertisementDiego BarreraNo ratings yet
- GAD Treatment OptionsDocument3 pagesGAD Treatment OptionsRosaNo ratings yet
- Citalopram - A Review of Pharmacological and CliniDocument15 pagesCitalopram - A Review of Pharmacological and CliniFirmansyahNo ratings yet
- Haad NotesDocument39 pagesHaad NotesBasicEdit CocoDurianNo ratings yet
- ZoloftDocument26 pagesZoloftgofastjayNo ratings yet
- Antidepressants Pharmacology LectureDocument19 pagesAntidepressants Pharmacology LectureHomman TommanNo ratings yet
- Janardhan Reddy 2017 Clinical Practice Guidelines ForDocument17 pagesJanardhan Reddy 2017 Clinical Practice Guidelines ForALISHA ARORANo ratings yet
- Lesson 6 - Anxiety-DisordersDocument74 pagesLesson 6 - Anxiety-DisordersKristian Dave DivaNo ratings yet
- Temple Grandin Autism and My Sensory Based World PDFDocument104 pagesTemple Grandin Autism and My Sensory Based World PDFΑυτιστικό Φάσμα Ε.Δ.Α.Α.Φ.100% (2)
- Anxiety Disorders in Children and AdolescentsDocument117 pagesAnxiety Disorders in Children and AdolescentsHendra SinagaNo ratings yet
- JCM 10 05912Document8 pagesJCM 10 05912Sandara SamperNo ratings yet
- Generalized Anxiety Disorder, Diagnosis and TreatmentDocument6 pagesGeneralized Anxiety Disorder, Diagnosis and TreatmentPaulus SidhartaNo ratings yet
- A Regulatory Apologia-A Review of Placebo-Controlled Studies in Regulatory Submissions of New-Generation Antidepressants - Melander 2008Document5 pagesA Regulatory Apologia-A Review of Placebo-Controlled Studies in Regulatory Submissions of New-Generation Antidepressants - Melander 2008Julio JuarezNo ratings yet
- Pharmacology Bullets (Nursing)Document2 pagesPharmacology Bullets (Nursing)Mariz Quidlat100% (2)
- Pharmacology Psychiatric MedicationsDocument36 pagesPharmacology Psychiatric Medicationsamasoud96 amasoud96No ratings yet
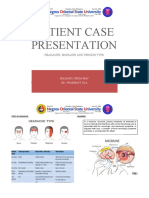
- Patient Case Presentation: Headache: Migraine and Tension TypeDocument31 pagesPatient Case Presentation: Headache: Migraine and Tension TypeKathleen B Baldado100% (4)
- Anxiety 2Document11 pagesAnxiety 2tela teliNo ratings yet
- Pharmacology and Toxicology of Antidepressants and AntipsychoticsDocument50 pagesPharmacology and Toxicology of Antidepressants and AntipsychoticsPintu Bhushan MitraNo ratings yet
- Depressive Disorders: PathophysiologyDocument19 pagesDepressive Disorders: Pathophysiology21613284No ratings yet
- Anti Anxiety MedicationsDocument2 pagesAnti Anxiety MedicationsjhgkhgkhgNo ratings yet
- Guide to Generic Drugs, Patents, and the Pharmaceutical MarketDocument28 pagesGuide to Generic Drugs, Patents, and the Pharmaceutical Marketjohn gringhamNo ratings yet
- Drugs:: Side Effects of Psychotropic MedicationsDocument32 pagesDrugs:: Side Effects of Psychotropic MedicationsMARIE ROSE L. FUNTANARNo ratings yet
- Postpartum BluesDocument8 pagesPostpartum Bluesbella kardinaNo ratings yet
- Dysthymia More Than "Minor" DepressionDocument5 pagesDysthymia More Than "Minor" DepressionNathaly BerríoNo ratings yet