You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Chest X-Ray InterpretationDocument30 pagesChest X-Ray InterpretationNuru99100% (19)
- Muscles of The Thorax That Assist in BreathingDocument6 pagesMuscles of The Thorax That Assist in Breathinge jeighNo ratings yet
- Electrocardiography (ECG)Document11 pagesElectrocardiography (ECG)Hassan AnwarNo ratings yet
- Pneumonia: Nur Yahya, T 05/1087561/KU/11522Document19 pagesPneumonia: Nur Yahya, T 05/1087561/KU/11522Taufik Nur YahyaNo ratings yet
- Cross Sectional Anatomy of SpineDocument37 pagesCross Sectional Anatomy of SpineAvinash Gupta50% (2)
- Pig Heart DissectionDocument4 pagesPig Heart Dissectiongerardgil82No ratings yet
- Valvular Heart DiseaseDocument54 pagesValvular Heart DiseaseRommanah AzmiNo ratings yet
- MCQ Ophthalmo WITH AnswersDocument3 pagesMCQ Ophthalmo WITH AnswersEddie Lim100% (1)
- MCQ Ophthalmo WITH AnswersDocument3 pagesMCQ Ophthalmo WITH AnswersEddie Lim100% (1)
- MCQ Ophthalmo WITH AnswersDocument3 pagesMCQ Ophthalmo WITH AnswersEddie Lim100% (1)
- MCQ Ophthalmo WITH AnswersDocument3 pagesMCQ Ophthalmo WITH AnswersEddie Lim100% (1)
- Topical Medication For GlaucomaDocument2 pagesTopical Medication For GlaucomaEddie LimNo ratings yet
- Checking Anaesthetic Equipment 2012Document18 pagesChecking Anaesthetic Equipment 2012Don David100% (1)
- Laboratory Tests of Renal Function PDFDocument4 pagesLaboratory Tests of Renal Function PDFEddie LimNo ratings yet
- Electrolytes Disorders in The Critically Ill PDFDocument6 pagesElectrolytes Disorders in The Critically Ill PDFEddie LimNo ratings yet
- Drugs and Renal Insufficiency PDFDocument3 pagesDrugs and Renal Insufficiency PDFEddie LimNo ratings yet
- 20 Easy Ways To Boost Your MemoryDocument5 pages20 Easy Ways To Boost Your MemoryEddie LimNo ratings yet
- HypertensionDocument1 pageHypertensionEddie LimNo ratings yet
- Human Heart Coloring Sheet With QR CodesDocument2 pagesHuman Heart Coloring Sheet With QR Codesapi-280337641No ratings yet
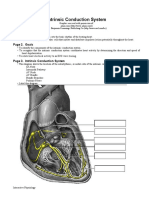
- Intrinsic Conduction System: Page 1. IntroductionDocument5 pagesIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNo ratings yet
- LUNG-OVERVIEW (Autosaved)Document132 pagesLUNG-OVERVIEW (Autosaved)Thivashinie Kandy Nazan VelloNo ratings yet
- Raquis CervicalDocument43 pagesRaquis Cervicalandrespineda12No ratings yet
- May 2012 Rounds Lung Basics PP PresentationDocument38 pagesMay 2012 Rounds Lung Basics PP PresentationNarulita putri hapsariNo ratings yet
- Axial Skeleton Study GuideDocument108 pagesAxial Skeleton Study GuideTheFTWPandaNo ratings yet
- Faktor Risiko Penyakit Jantung Koroner Di RSI SITI Khadijah PalembangDocument6 pagesFaktor Risiko Penyakit Jantung Koroner Di RSI SITI Khadijah PalembangYanis HildaNo ratings yet
- Ebstein Anomaly in The Adult PatientDocument11 pagesEbstein Anomaly in The Adult PatientRJMNo ratings yet
- ArticleDocument4 pagesArticleapi-629928343No ratings yet
- How To Perform A Transseptal Puncture: Mark J EarleyDocument9 pagesHow To Perform A Transseptal Puncture: Mark J EarleyAttilio Del RossoNo ratings yet
- Week 29-Angina - MI PDFDocument7 pagesWeek 29-Angina - MI PDFJaimie Charlotte Marie LangilleNo ratings yet
- Kerala University of Health Sciences (Kuhs) Expected Questions On First Year BSC Nursing Degree Examinations 2021Document5 pagesKerala University of Health Sciences (Kuhs) Expected Questions On First Year BSC Nursing Degree Examinations 2021ashna anilNo ratings yet
- Cervical Vertebrae Print Page - Unlabeled Diagram (Image) and TextDocument3 pagesCervical Vertebrae Print Page - Unlabeled Diagram (Image) and TextNourhan JamalNo ratings yet
- TOPIC 12 The Cardiovascular SystemDocument27 pagesTOPIC 12 The Cardiovascular SystemLorraine RiegoNo ratings yet
- Circulatory System SummaryDocument3 pagesCirculatory System SummaryNiel S. DefensorNo ratings yet
- Scans en 2015Document43 pagesScans en 2015Carolina Duque RodriguezNo ratings yet
- Echocardiography Dissertation IdeasDocument8 pagesEchocardiography Dissertation IdeasWhoCanWriteMyPaperForMeCanada100% (1)
- Anatomy of The Thoracic Wall, Pulmonary Cavities, and MediastinumDocument26 pagesAnatomy of The Thoracic Wall, Pulmonary Cavities, and Mediastinumearly intervention centre thudiylu trerNo ratings yet
- Mitral StenosisDocument17 pagesMitral Stenosispriyanka bhowmikNo ratings yet
- Laboratory 3 - Blood Vessels I - Histology of Artery and Vein ArteriesDocument28 pagesLaboratory 3 - Blood Vessels I - Histology of Artery and Vein ArteriesSofia NNo ratings yet
- G Transport (Animals II)Document8 pagesG Transport (Animals II)mjNo ratings yet
- Heart IntroductionDocument16 pagesHeart Introductionsentilbalan@gmail.comNo ratings yet
- K - 12 Heart As A Pump (Fisiologi)Document36 pagesK - 12 Heart As A Pump (Fisiologi)missirenaNo ratings yet