You might also like
- Holistic Pregnancy Manual: Maternal Health Manuals, #1From EverandHolistic Pregnancy Manual: Maternal Health Manuals, #1No ratings yet
- Latent Phase of LabourDocument10 pagesLatent Phase of LabourFELIX CLINENo ratings yet
- Pregnancy, Birth and Beyond: A Spiritual and Practical GuideFrom EverandPregnancy, Birth and Beyond: A Spiritual and Practical GuideNo ratings yet
- Pre Labor VsDocument6 pagesPre Labor VsMarffy Llamas100% (1)
- Holistic Postpartum Manual: Maternal Health Manuals, #3From EverandHolistic Postpartum Manual: Maternal Health Manuals, #3No ratings yet
- All About PragnancyDocument29 pagesAll About PragnancyBaalu KathirveluNo ratings yet
- Antenatal Info Booklet Intuitive BirthDocument32 pagesAntenatal Info Booklet Intuitive Birthapi-223713414No ratings yet
- The Earliest Weeks of PregnancyDocument23 pagesThe Earliest Weeks of PregnancyAnaleah MalayaoNo ratings yet
- Labor Delivery TipsDocument32 pagesLabor Delivery TipsAivvee DraculanNo ratings yet
- 9th Month of PregnancyDocument2 pages9th Month of PregnancyVicky OZNo ratings yet
- Birth Course Companion Ebook-3Document97 pagesBirth Course Companion Ebook-3shivanibatraNo ratings yet
- Lending LibraryDocument1 pageLending Libraryapi-247440750No ratings yet
- Welcoming The Maiden Archetype: When Can I Do The Meditation?Document3 pagesWelcoming The Maiden Archetype: When Can I Do The Meditation?Gabrijela TominacNo ratings yet
- The Motherly Guide To Becoming MamaDocument10 pagesThe Motherly Guide To Becoming Mamaamstelbryan39No ratings yet
- Amounts of Foods To OfferDocument1 pageAmounts of Foods To OfferMadalin PlastoiNo ratings yet
- FPQC Positions For LaborDocument3 pagesFPQC Positions For LaborAukia HyuugaNo ratings yet
- Pregnancy Options Book A5 Website 1Document33 pagesPregnancy Options Book A5 Website 1api-252780946No ratings yet
- HandoutmassageDocument1 pageHandoutmassageapi-244719696No ratings yet
- Why Home Birth Is NecessaryDocument3 pagesWhy Home Birth Is NecessaryMutiara Ummu SumayyahNo ratings yet
- L&D Worksheet Student SampleDocument3 pagesL&D Worksheet Student Sampleth233No ratings yet
- Month by MonthDocument28 pagesMonth by MonthChoi Han KimNo ratings yet
- Pregnancy OptionsDocument116 pagesPregnancy OptionsBharti CartesNo ratings yet
- 21 Day Detox RecipesDocument41 pages21 Day Detox Recipesphilippe28790No ratings yet
- Handout 5 PDFDocument4 pagesHandout 5 PDFApRil Anne BalanonNo ratings yet
- Ceremony - Candle Lighting PDFDocument2 pagesCeremony - Candle Lighting PDFrafaelgsccNo ratings yet
- Doulas and Labor SupportDocument2 pagesDoulas and Labor SupportbatlixieNo ratings yet
- Pregnancy Stages GuideDocument15 pagesPregnancy Stages Guidefarhan_ansNo ratings yet
- PHD Student: Thierry Claudien Uhawenimana Supervisors: Prof. Alison Mcfadden, Dr. Nicola Gray, Dr. Heather WhitfordDocument1 pagePHD Student: Thierry Claudien Uhawenimana Supervisors: Prof. Alison Mcfadden, Dr. Nicola Gray, Dr. Heather WhitfordThierry UhawenimanaNo ratings yet
- Natural FertilityDocument148 pagesNatural FertilityAish LakshNo ratings yet
- Labor and Birth HandoutDocument9 pagesLabor and Birth Handoutapi-240665032No ratings yet
- Lamaze 6healthybirthpractices Infographic FinalDocument1 pageLamaze 6healthybirthpractices Infographic Finalapi-264859193No ratings yet
- BCC Session3 LinksextrasDocument13 pagesBCC Session3 Linksextrasapi-222516709No ratings yet
- Chakra Balancing GuideDocument4 pagesChakra Balancing Guidesvp3761No ratings yet
- Easy Steps To A Safer PregnancyDocument53 pagesEasy Steps To A Safer PregnancySummer Time100% (1)
- Leopolds Manuever Final 21aDocument27 pagesLeopolds Manuever Final 21aArun Roa DanielNo ratings yet
- Clinical Week 3 - Teaching Plan - BreastfeedingDocument2 pagesClinical Week 3 - Teaching Plan - Breastfeedingapi-273168705No ratings yet
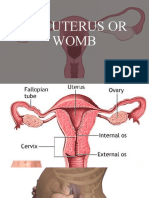
- The Uterus or WombDocument38 pagesThe Uterus or WombmuwahNo ratings yet
- Labor and Delivery TopicsDocument44 pagesLabor and Delivery TopicsAngela Joy AmparadoNo ratings yet
- Fetal MalpresentationDocument33 pagesFetal MalpresentationMichael Angelo Seña100% (1)
- Lunar Chart GuideDocument9 pagesLunar Chart GuideElena M100% (1)
- Antenatal Care Schedule Handout - GP Low Risk May 2018Document4 pagesAntenatal Care Schedule Handout - GP Low Risk May 2018maddy100% (1)
- Meditation Har Trust in GodDocument3 pagesMeditation Har Trust in GodNicole HawkinsNo ratings yet
- Lotus BirthDocument4 pagesLotus BirthindahNo ratings yet
- Pregnancy Yoga Postures For LabourDocument29 pagesPregnancy Yoga Postures For LabourAjay IyerNo ratings yet
- BCC Session2 LinksextrasDocument6 pagesBCC Session2 Linksextrasapi-222516709No ratings yet
- The Postpartum TraditionDocument24 pagesThe Postpartum TraditionAzher Hameed QamarNo ratings yet
- Module 6 IntrapartumDocument33 pagesModule 6 IntrapartumTiangco Fatima AlfaNo ratings yet
- FAKE FAKE Document - Please Don't Use This: Associated Body PartsDocument18 pagesFAKE FAKE Document - Please Don't Use This: Associated Body Partsgnk1975No ratings yet
- Nursing Mothers GuideDocument11 pagesNursing Mothers GuidepbanerjeeNo ratings yet
- Relaxation Techniques for Labor Pain ReliefDocument23 pagesRelaxation Techniques for Labor Pain ReliefEdderlyn LamarcaNo ratings yet
- The Menstrual Cycle WorksheetDocument2 pagesThe Menstrual Cycle Worksheetapi-383924075% (4)
- Anatomical and Physiological Changes During PregnancyDocument25 pagesAnatomical and Physiological Changes During Pregnancyqaleeq100% (1)
- NWHRC - Pregnancyplanner Your GuideDocument16 pagesNWHRC - Pregnancyplanner Your GuideRiyan WahyudoNo ratings yet
- Birth Partners' Affirmations Script..Document6 pagesBirth Partners' Affirmations Script..nadyaNo ratings yet
- Impact of Doulas Delivery and BFDocument10 pagesImpact of Doulas Delivery and BFFabiola AndreaNo ratings yet
- Ebook Vaginal SteamingDocument14 pagesEbook Vaginal SteamingDana DragomirescuNo ratings yet
- Managing Pain During Childbirth With Massage, Reflexology and Other Manual MethodsDocument11 pagesManaging Pain During Childbirth With Massage, Reflexology and Other Manual MethodsFiraNo ratings yet
- Essential Perinatal Exercises for Strength and FlexibilityDocument12 pagesEssential Perinatal Exercises for Strength and FlexibilityJeane Rose PurazoNo ratings yet
- Pelvic Girdle Pain Fact SheetDocument5 pagesPelvic Girdle Pain Fact SheetagniosaiNo ratings yet
- Formulation and Evaluation of Antiseptic Polyherbal OintmentDocument11 pagesFormulation and Evaluation of Antiseptic Polyherbal OintmentandrapradeshsseNo ratings yet
- MedicalDocument3 pagesMedicalmumtazkauser74No ratings yet
- Case Report in Psychiatry051.03Document4 pagesCase Report in Psychiatry051.03Christian Tan Getana100% (1)
- Med Surge 2 Mod 3 Study GuideDocument19 pagesMed Surge 2 Mod 3 Study GuideDirk Buckner100% (4)
- Mycoplasma Genitalium A4Document1 pageMycoplasma Genitalium A4Nauli NasirNo ratings yet
- Current Status of NTD PhilippinesDocument28 pagesCurrent Status of NTD PhilippinesMelody PardilloNo ratings yet
- Brand Name Generic Name Disease Group Consumer Medicine Information More InfoDocument9 pagesBrand Name Generic Name Disease Group Consumer Medicine Information More InfoBairavi RathakrishnanNo ratings yet
- The Nursing Process: Dr. Abdalkarim RadwanDocument62 pagesThe Nursing Process: Dr. Abdalkarim RadwanAngelique Ramos PascuaNo ratings yet
- Nursing Care of Clients with Physiologic and Psychosocial AlterationsDocument14 pagesNursing Care of Clients with Physiologic and Psychosocial AlterationsBrianMarBeltran100% (1)
- Stress Management in StudentsDocument25 pagesStress Management in StudentsJangNo ratings yet
- Measuring Lung Capacity PDFDocument5 pagesMeasuring Lung Capacity PDFSip BioNo ratings yet
- Leptin HormoneDocument21 pagesLeptin Hormonemarah almahameed100% (2)
- Varicose Vein SurgeryDocument11 pagesVaricose Vein SurgeryDaud YudhistiraNo ratings yet
- NCP Pancreatic MassDocument4 pagesNCP Pancreatic MassJan Lianne BernalesNo ratings yet
- CROSSBITE According To GraberDocument29 pagesCROSSBITE According To GraberAslamCv100% (1)
- Nerve Cell - Cell ProjectDocument23 pagesNerve Cell - Cell Projectapi-327766139No ratings yet
- Unstable Angina Case ReportDocument24 pagesUnstable Angina Case ReportaybatariNo ratings yet
- Thoughts Thoughts: 'Universe, Please Help Me Maintain An Effective Meditative-State. Thank You.'Document4 pagesThoughts Thoughts: 'Universe, Please Help Me Maintain An Effective Meditative-State. Thank You.'Mincheol KangNo ratings yet
- Nurs 205 Concept MapDocument1 pageNurs 205 Concept MapJami SpearsNo ratings yet
- Twins Bootcamp StudyDocument5 pagesTwins Bootcamp Studyandi dirhanNo ratings yet
- Nucleus DropDocument1 pageNucleus DropYovinus DenyNo ratings yet
- Varicella in Pregnancy GuidelineDocument5 pagesVaricella in Pregnancy GuidelineYwagar YwagarNo ratings yet
- Review On Surge Drug Delivery TechnologyDocument8 pagesReview On Surge Drug Delivery TechnologyNayeli MercadoNo ratings yet
- 13 Implant Supported Fixed ProsthesesDocument52 pages13 Implant Supported Fixed ProsthesesJúliaJulieNo ratings yet
- Practicing The A, B, C'S: Albert Ellis and REBTDocument24 pagesPracticing The A, B, C'S: Albert Ellis and REBTShareenjitKaurNo ratings yet
- A Critical Examination of The Homeopathic Treatment of Chronic Fatigue SyndromeDocument18 pagesA Critical Examination of The Homeopathic Treatment of Chronic Fatigue SyndromeceliastNo ratings yet
- Shiatsu Helps Treat AsthmaDocument9 pagesShiatsu Helps Treat Asthmaडा. सत्यदेव त्यागी आर्यNo ratings yet
- WREBDocument94 pagesWREBJessica Bahga100% (1)
- Topical and Structurated Syllabus Corrected.1Document10 pagesTopical and Structurated Syllabus Corrected.1Kikis Dom100% (1)
- Guidelines Antibiotic Step-Down TherapyDocument1 pageGuidelines Antibiotic Step-Down TherapyGayle GreyNo ratings yet
- Chakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.From EverandChakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.Rating: 4 out of 5 stars4/5 (2)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Hero Maker: 12 Weeks to Superhero Fit: A Hollywood Trainer's REAL Guide to Getting the Body You've Always WantedFrom EverandHero Maker: 12 Weeks to Superhero Fit: A Hollywood Trainer's REAL Guide to Getting the Body You've Always WantedRating: 4 out of 5 stars4/5 (1)
- The Yogi Code: Seven Universal Laws of Infinite SuccessFrom EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessRating: 4.5 out of 5 stars4.5/5 (104)
- Calisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesFrom EverandCalisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesRating: 3 out of 5 stars3/5 (5)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (780)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindFrom EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindRating: 4.5 out of 5 stars4.5/5 (1)
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerFrom EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerRating: 4 out of 5 stars4/5 (5)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!From EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Rating: 4.5 out of 5 stars4.5/5 (22)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsFrom EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsRating: 5 out of 5 stars5/5 (95)
- Wall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesFrom EverandWall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesNo ratings yet
- 7 Weeks to 10 Pounds of Muscle: The Complete Day-by-Day Program to Pack on Lean, Healthy Muscle MassFrom Everand7 Weeks to 10 Pounds of Muscle: The Complete Day-by-Day Program to Pack on Lean, Healthy Muscle MassRating: 4 out of 5 stars4/5 (2)
- If You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsFrom EverandIf You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsRating: 4.5 out of 5 stars4.5/5 (7)
- SAS Training Manual: How to get fit enough to pass a special forces selection courseFrom EverandSAS Training Manual: How to get fit enough to pass a special forces selection courseRating: 4 out of 5 stars4/5 (3)
- Meat Is for Pussies: A How-To Guide for Dudes Who Want to Get Fit, Kick Ass, and Take NamesFrom EverandMeat Is for Pussies: A How-To Guide for Dudes Who Want to Get Fit, Kick Ass, and Take NamesRating: 3.5 out of 5 stars3.5/5 (8)
- Body by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekFrom EverandBody by Science: A Research Based Program for Strength Training, Body building, and Complete Fitness in 12 Minutes a WeekRating: 4.5 out of 5 stars4.5/5 (84)
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (110)
- Slow Burn: Burn Fat Faster By Exercising SlowerFrom EverandSlow Burn: Burn Fat Faster By Exercising SlowerRating: 4.5 out of 5 stars4.5/5 (6)
- ROAR: How to Match Your Food and Fitness to Your Unique Female Physiology for Optimum Performance, Great Health, and a Strong, Lean Body for LifeFrom EverandROAR: How to Match Your Food and Fitness to Your Unique Female Physiology for Optimum Performance, Great Health, and a Strong, Lean Body for LifeRating: 4.5 out of 5 stars4.5/5 (44)
- Applied Polyvagal Theory in Yoga: Therapeutic Practices for Emotional HealthFrom EverandApplied Polyvagal Theory in Yoga: Therapeutic Practices for Emotional HealthNo ratings yet
- Beastmode Calisthenics: A Simple and Effective Guide to Get Ripped with Bodyweight TrainingFrom EverandBeastmode Calisthenics: A Simple and Effective Guide to Get Ripped with Bodyweight TrainingNo ratings yet
- Light on Yoga: The Definitive Guide to Yoga PracticeFrom EverandLight on Yoga: The Definitive Guide to Yoga PracticeRating: 5 out of 5 stars5/5 (1)
- Calisthenics: 12 Effective Exercises to Build Calisthenics Body in 14 DaysFrom EverandCalisthenics: 12 Effective Exercises to Build Calisthenics Body in 14 DaysRating: 3 out of 5 stars3/5 (5)
- The Calisthenics Codex: Fifty Exercises for Functional FitnessFrom EverandThe Calisthenics Codex: Fifty Exercises for Functional FitnessRating: 4 out of 5 stars4/5 (9)
- 7 Weeks to 50 Pull-Ups: Strengthen and Sculpt Your Arms, Shoulders, Back, and Abs by Training to Do 50 Consecutive Pull-UpsFrom Everand7 Weeks to 50 Pull-Ups: Strengthen and Sculpt Your Arms, Shoulders, Back, and Abs by Training to Do 50 Consecutive Pull-UpsRating: 3.5 out of 5 stars3.5/5 (2)
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingFrom EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingRating: 4.5 out of 5 stars4.5/5 (19)
- The Professional Yoga Teacher's Handbook: The Ultimate Guide for Current and Aspiring Instructors?Set Your Intention, Develop Your Voice, and Build Your CareerFrom EverandThe Professional Yoga Teacher's Handbook: The Ultimate Guide for Current and Aspiring Instructors?Set Your Intention, Develop Your Voice, and Build Your CareerRating: 5 out of 5 stars5/5 (2)