You might also like
- Fundamentals Workbook ENG RevDocument25 pagesFundamentals Workbook ENG RevottozirgNo ratings yet
- Many Mindfulness Exercises: Patricia Bear, LPCDocument6 pagesMany Mindfulness Exercises: Patricia Bear, LPCAna LeahNo ratings yet
- Respiratory System: Anatomy & PhysiologyDocument111 pagesRespiratory System: Anatomy & PhysiologyJape GarridoNo ratings yet
- The Miracle of Manaforce PowerDocument26 pagesThe Miracle of Manaforce PowerenekosaaneNo ratings yet
- Simple MeditationDocument2 pagesSimple MeditationDr.ManageNo ratings yet
- Respiratory System (Anatomy and Physiology)Document71 pagesRespiratory System (Anatomy and Physiology)Butch Dumdum100% (11)
- Physiotherapy in Respiratory Care 3rd Ed - A. Hough (Nelson Thornes, 2001) WW PDFDocument562 pagesPhysiotherapy in Respiratory Care 3rd Ed - A. Hough (Nelson Thornes, 2001) WW PDFDaria Nectaria100% (1)
- Shen Gong Exercises PDFDocument3 pagesShen Gong Exercises PDFRahimNo ratings yet
- The Human Respiratory SystemDocument15 pagesThe Human Respiratory SystemNandita Halder100% (1)
- MCQ Exam 2011 PDFDocument22 pagesMCQ Exam 2011 PDFBranka Kurtovic80% (10)
- Anatomy of Respiratory SystemDocument57 pagesAnatomy of Respiratory SystemRyan Larsen100% (1)
- OxygenationDocument20 pagesOxygenationKhie-An OcampoNo ratings yet
- HaraShiatsu Self HealingDocument3 pagesHaraShiatsu Self HealingAWEDIOHEADNo ratings yet
- Anaesthesia Breathing CircuitsDocument8 pagesAnaesthesia Breathing CircuitsSuresh KumarNo ratings yet
- Respiratory System Anatomy, Assessment & Diagnostic TestsDocument24 pagesRespiratory System Anatomy, Assessment & Diagnostic TestsPrince Rener Velasco PeraNo ratings yet
- Respiratory SystemDocument32 pagesRespiratory Systemapi-202513022No ratings yet
- NursingBulletin Respiratory SystemDocument35 pagesNursingBulletin Respiratory Systemseigelystic100% (3)
- Pear Cone WaveDocument2 pagesPear Cone WaveMichael Grant White100% (2)
- The Respiratory SystemDocument147 pagesThe Respiratory SystemAya SobhiNo ratings yet
- Alexander Breathing Pain ReliefDocument2 pagesAlexander Breathing Pain ReliefSyedNo ratings yet
- Anatomy and Physiology: The Respiratory SystemDocument82 pagesAnatomy and Physiology: The Respiratory SystemMaria Angelique Ofciar100% (2)
- Anatomy of Respiratory System: Dr. Dwi Rita Anggraini, MkesDocument64 pagesAnatomy of Respiratory System: Dr. Dwi Rita Anggraini, MkesFira TasyaNo ratings yet
- Anatomy and Physiology of The Respiratory SystemDocument5 pagesAnatomy and Physiology of The Respiratory SystemxoxosvwNo ratings yet
- Respiratory Physiology AnswersDocument4 pagesRespiratory Physiology AnswersRamya100% (3)
- Group1 Review of Respiratory SystemDocument41 pagesGroup1 Review of Respiratory Systemjohn obinaNo ratings yet
- Respiratory System s2 2019Document56 pagesRespiratory System s2 2019noviantyramadhani12No ratings yet
- 22 Respiratory SystemDocument99 pages22 Respiratory SystemvanderphysNo ratings yet
- The Respiratory System: ASTIKA NUR ROHMAH, S.Kep., NS., M.BiomedDocument43 pagesThe Respiratory System: ASTIKA NUR ROHMAH, S.Kep., NS., M.BiomedAdek KhazeliaNo ratings yet
- Respiratory NotesDocument6 pagesRespiratory NotesBethany CrawfordNo ratings yet
- Respiratory SystemDocument53 pagesRespiratory SystemRotan CirebonNo ratings yet
- Physiology of The Respiratory System-1Document155 pagesPhysiology of The Respiratory System-1Adil MusaddiqNo ratings yet
- Self Test 3Document6 pagesSelf Test 3202310446No ratings yet
- Week 3 Respiratory SystemDocument10 pagesWeek 3 Respiratory SystemangeliaNo ratings yet
- 1.anatomy of Respiratory SystemDocument73 pages1.anatomy of Respiratory Systemokoti.omutanyi22No ratings yet
- Lecture 5 Respiratory System 1Document61 pagesLecture 5 Respiratory System 1hafiz patahNo ratings yet
- Anatomi Sistem ParuDocument64 pagesAnatomi Sistem ParuMochammad Fariz AmsalNo ratings yet
- Respiratory SystemDocument12 pagesRespiratory Systemab4943409No ratings yet
- Anatomy, Physiology and Pathology of The RespiratoryDocument68 pagesAnatomy, Physiology and Pathology of The Respiratorytheresia_s_k100% (1)
- Anatomy of The Respiratory SystemDocument37 pagesAnatomy of The Respiratory SystemPal SedNo ratings yet
- Respiratory System Anatomy and Physiology: Marianne Belleza, RNDocument18 pagesRespiratory System Anatomy and Physiology: Marianne Belleza, RNTiara GustiwiyanaNo ratings yet
- Respiratory SystemDocument9 pagesRespiratory SystemShivani Sriram100% (1)
- RESPIRATORY DISTURBANCES - HandoutsDocument35 pagesRESPIRATORY DISTURBANCES - Handoutsfebie pachecoNo ratings yet
- NCM 112 LEC Topic 1 Respiratory System Anatomy PhysiologyDocument7 pagesNCM 112 LEC Topic 1 Respiratory System Anatomy PhysiologyViviene Faye FombuenaNo ratings yet
- Respiratory Tract Structure: Alveolus)Document5 pagesRespiratory Tract Structure: Alveolus)MarekGojtowskiNo ratings yet
- UntitledDocument62 pagesUntitledManaye MamuyeNo ratings yet
- Lecture - 5 PDFDocument5 pagesLecture - 5 PDFDavid JokerNo ratings yet
- ANAPHYDocument10 pagesANAPHYcharles babasaNo ratings yet
- Respiratory SystemDocument5 pagesRespiratory SystemPreeti ChouhanNo ratings yet
- Module 4 Respiratory SystemDocument8 pagesModule 4 Respiratory SystemJake Donely C. PaduaNo ratings yet
- Anatomy 2nd-U-3 Respiratory SystemDocument113 pagesAnatomy 2nd-U-3 Respiratory Systemsinte beyuNo ratings yet
- 1-Respiratory MechanicsDocument56 pages1-Respiratory MechanicsDoha JKNo ratings yet
- Respiratory System PDFDocument16 pagesRespiratory System PDFMary Ann SacramentoNo ratings yet
- The Respiratory System PP First - Stage 2021Document27 pagesThe Respiratory System PP First - Stage 2021HHHNo ratings yet
- Respiratory SystemDocument5 pagesRespiratory SystemКрістіна БаландаNo ratings yet
- Respiratory System - Anatomy and PhysiologyDocument6 pagesRespiratory System - Anatomy and PhysiologyJay Crishnan Morales CajandingNo ratings yet
- Functional Anatomy of The Respiratory System NoseDocument5 pagesFunctional Anatomy of The Respiratory System NoseEjie Boy IsagaNo ratings yet
- Respiratory System: Sakina Dept. Anatomi Dan Histologi FK UnairDocument52 pagesRespiratory System: Sakina Dept. Anatomi Dan Histologi FK UnairFhyrha MyuceNo ratings yet
- ScienceDocument14 pagesSciencesheanellerenzsantosNo ratings yet
- Respiratory SystemDocument5 pagesRespiratory SystemrianaNo ratings yet
- Lec:2 Respiratory System DR - HudaDocument4 pagesLec:2 Respiratory System DR - HudaLina AyadNo ratings yet
- Respiratory System 1 Physiology 16-11-2018Document25 pagesRespiratory System 1 Physiology 16-11-2018Kangwa MasekaNo ratings yet
- Anatomy and Physiology of Respiratory SystemDocument4 pagesAnatomy and Physiology of Respiratory Systembilliam123No ratings yet
- Human Biology: Respiratory SystemDocument33 pagesHuman Biology: Respiratory SystemSaikrishna RaoNo ratings yet
- Anatomy & PhysiologyDocument42 pagesAnatomy & PhysiologyArah Lyn ApiagNo ratings yet
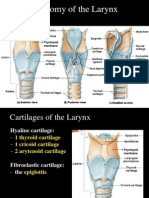
- Anatomy of The Larynx: Thyrohyoid MembraneDocument35 pagesAnatomy of The Larynx: Thyrohyoid MembraneVarsha Shende KhobragadeNo ratings yet
- Respiratory & Urinary System 1Document3 pagesRespiratory & Urinary System 1Ishmael DimagibaNo ratings yet
- PAin and Oxygenation HandoutsPRELIMSDocument7 pagesPAin and Oxygenation HandoutsPRELIMSJhoanna de ChavezNo ratings yet
- Functions of The Respiratory SystemDocument10 pagesFunctions of The Respiratory SystemKrisha AvorqueNo ratings yet
- Functional Human Physiology: The Respiratory SystemDocument64 pagesFunctional Human Physiology: The Respiratory SystemnashqonashNo ratings yet
- Respiratory System Semi FinalDocument60 pagesRespiratory System Semi FinalMichelle AnteneroNo ratings yet
- How Do Humans Breathe? Science Book Age 8 | Children's Biology BooksFrom EverandHow Do Humans Breathe? Science Book Age 8 | Children's Biology BooksNo ratings yet
- Apa Itu MengikDocument2 pagesApa Itu MengikAmy Tryabto ArifinNo ratings yet
- Dental Human PhysiologyDocument148 pagesDental Human Physiologypawi18No ratings yet
- 10th Biology Guess 2019Document5 pages10th Biology Guess 2019muhammad zulqarnainNo ratings yet
- CSEC Biology January 2007 042Document8 pagesCSEC Biology January 2007 042Makayla AlexanderNo ratings yet
- Ewquickguide 2 EdDocument188 pagesEwquickguide 2 EdStanley Wu TaiNo ratings yet
- Definisi Dan Terapi - Id.enDocument11 pagesDefinisi Dan Terapi - Id.enCindy Ari SantiNo ratings yet
- 10bja Medsci - Mckenzie CheyneDocument60 pages10bja Medsci - Mckenzie Cheyneapi-284323075No ratings yet
- KA THA RA HEALING STEP ONE - Awakening The MENTOR & 6th & 7th SensesDocument5 pagesKA THA RA HEALING STEP ONE - Awakening The MENTOR & 6th & 7th SensesfarahNo ratings yet
- Patient-Ventilator Dyssynchrony in The Intensive Care Unit A PracticalDocument12 pagesPatient-Ventilator Dyssynchrony in The Intensive Care Unit A PracticalBrenda Serrano LaraNo ratings yet
- RespirationDocument6 pagesRespirationAbu BeastNo ratings yet
- Marieb 2015 11th 0321919009 SampleDocument31 pagesMarieb 2015 11th 0321919009 SampleJoe Chill100% (1)
- Ebook Pulmonary Physiology Tenth Edition PDF Full Chapter PDFDocument67 pagesEbook Pulmonary Physiology Tenth Edition PDF Full Chapter PDFbobby.bianco575100% (25)
- Box Breathing PDFDocument8 pagesBox Breathing PDFScribd AnonNo ratings yet
- Alteration in Respiratory SystemDocument138 pagesAlteration in Respiratory Systemcute_gurljhoanNo ratings yet
- GR-5 ScienceDocument354 pagesGR-5 SciencePrecious RubaNo ratings yet
- BBBBBBNNNDocument6 pagesBBBBBBNNNIrfana EfendiNo ratings yet
- Medtronic PB560 - 10039030M00 - PB560 SYSTEM FINAL TEST PROCEDUREDocument12 pagesMedtronic PB560 - 10039030M00 - PB560 SYSTEM FINAL TEST PROCEDUREDaniel MarquesNo ratings yet
- Forced Smoking Stories I'Ve CollectedDocument241 pagesForced Smoking Stories I'Ve CollectedErnesto PazNo ratings yet