You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Essential Notes in Pain MedicineDocument737 pagesEssential Notes in Pain MedicineRichard Pertwee100% (5)
- (Medical Psychiatry 29) Borwin Bandelow, Dan J. Stein - Social Anxiety Disorder-Marcel Dekker (2004) PDFDocument347 pages(Medical Psychiatry 29) Borwin Bandelow, Dan J. Stein - Social Anxiety Disorder-Marcel Dekker (2004) PDFmaria100% (1)
- Sci-Doku Chips LongDocument4 pagesSci-Doku Chips LongDave Remerata100% (2)
- Pharmacology of Phenadoxone dN-Morpholino 4:4 Diphenyl: HydrochlorideDocument17 pagesPharmacology of Phenadoxone dN-Morpholino 4:4 Diphenyl: Hydrochlorideisaev201No ratings yet
- Adderall-Safer Than AspirinDocument2 pagesAdderall-Safer Than AspirinChristopher RhudyNo ratings yet
- Karnofsky Performance Scale IndexDocument6 pagesKarnofsky Performance Scale IndexAmolkumar W DiwanNo ratings yet
- Kimuras - Disease Unusual Cause of Cervical TumorDocument4 pagesKimuras - Disease Unusual Cause of Cervical TumorAmolkumar W DiwanNo ratings yet
- Pleural DiseasesDocument52 pagesPleural DiseasesAmolkumar W DiwanNo ratings yet
- Conditions of Respi SystemDocument20 pagesConditions of Respi SystemAmolkumar W DiwanNo ratings yet
- Burden of Disease in India NCMCHDocument388 pagesBurden of Disease in India NCMCHBrand Synapse100% (1)
- Epidemiology of Childhood AsthmaDocument4 pagesEpidemiology of Childhood AsthmaAmolkumar W DiwanNo ratings yet
- Herb A LifeDocument97 pagesHerb A LifeAmolkumar W DiwanNo ratings yet
- Respiratory Diseases Green Facts Level2Document11 pagesRespiratory Diseases Green Facts Level2Amolkumar W DiwanNo ratings yet
- TB MCQ UseDocument12 pagesTB MCQ UseAmolkumar W Diwan100% (6)
- Cellular Respiration: Food ATPDocument43 pagesCellular Respiration: Food ATPAmolkumar W DiwanNo ratings yet
- Depression in Older AdultsDocument9 pagesDepression in Older Adultsapi-509881562No ratings yet
- Diagnosis of Midface Fractures With CT: What The Surgeon Needs To KnowDocument24 pagesDiagnosis of Midface Fractures With CT: What The Surgeon Needs To KnowMohammad AdhityaNo ratings yet
- Test Bank For Clinical Immunology and Serology A Laboratory Perspective 3rd Edition StevensDocument11 pagesTest Bank For Clinical Immunology and Serology A Laboratory Perspective 3rd Edition StevensWilbur Penny100% (35)
- Drug StudyDocument4 pagesDrug StudyAilah Mae Dela Cruz0% (1)
- Mouth Sores Pictures, Causes, Types, Symptoms, and TreatmentsDocument1 pageMouth Sores Pictures, Causes, Types, Symptoms, and Treatmentslashes everafterNo ratings yet
- ExamView - Chapter - 33 PDFDocument8 pagesExamView - Chapter - 33 PDFChizua OkoyeNo ratings yet
- Nursing Procedure Manual Nobel Medical College Teaching Hospital Biratnager, NepalDocument334 pagesNursing Procedure Manual Nobel Medical College Teaching Hospital Biratnager, NepalSweta ManandharNo ratings yet
- LungRADS 1-1 UpdatesDocument13 pagesLungRADS 1-1 UpdatesMarcelNo ratings yet
- LoadVoucher AspxDocument4 pagesLoadVoucher AspxEdnalyn CasasNo ratings yet
- 3 - Whooping Cough and DiptheriaDocument25 pages3 - Whooping Cough and DiptheriaBa MulengaNo ratings yet
- Somatom Definition Edge Brochure-00024835Document56 pagesSomatom Definition Edge Brochure-00024835manuel pilco riosNo ratings yet
- HPEX 358-002 - Basics of EpidemiologyDocument31 pagesHPEX 358-002 - Basics of EpidemiologyMichelle ValenzuelaNo ratings yet
- nsg-320cc Care Plan 1Document14 pagesnsg-320cc Care Plan 1api-509452165No ratings yet
- PediatricDocument2 pagesPediatricDrNoor MD MohsenNo ratings yet
- Hemoflagellates TableDocument4 pagesHemoflagellates TableAbd Al Kareem RashedNo ratings yet
- Atomy IndiaDocument4 pagesAtomy IndiamaheshNo ratings yet
- Local AnestheticsDocument47 pagesLocal AnestheticsKeerthi LakshmiNo ratings yet
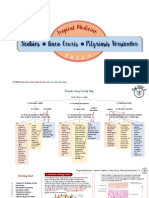
- Scabies Tinea Cruris Pityriasis Versicolor: Semangat!Document11 pagesScabies Tinea Cruris Pityriasis Versicolor: Semangat!Fitriah Nur SyamiatiNo ratings yet
- Classic Radiology SignsDocument9 pagesClassic Radiology SignsJui DirDapNo ratings yet
- B Blab 6 Crossmatch SP 05Document14 pagesB Blab 6 Crossmatch SP 05Rutchelle Joyce PugoyNo ratings yet
- Australian Dental Journal - 2015 - Ettinger - Treatment Planning Concepts For The Ageing PatientDocument15 pagesAustralian Dental Journal - 2015 - Ettinger - Treatment Planning Concepts For The Ageing PatientLorri - Ann LamontNo ratings yet
- Lecture 4 Diagnosis of Dental CariesDocument12 pagesLecture 4 Diagnosis of Dental CariesDt omarNo ratings yet
- Canine and Feline CryptorchidismDocument4 pagesCanine and Feline CryptorchidismkoloraNo ratings yet
- M4 - Didactic - NCM 118Document4 pagesM4 - Didactic - NCM 118KARL FESARITNo ratings yet
- Behandlingstudier - Overblik Over Planlagte Og Igangværende Studier Af Lægemidler Til Behandling Af COVID-19Document217 pagesBehandlingstudier - Overblik Over Planlagte Og Igangværende Studier Af Lægemidler Til Behandling Af COVID-19Ishan ShahNo ratings yet