You might also like
- InFlam ArthritisDocument53 pagesInFlam ArthritisMithun CbNo ratings yet
- Approach To Arthritis PDFDocument54 pagesApproach To Arthritis PDFanahitshoNo ratings yet
- Competency Based Training Programme: DNB-RheumatologyDocument34 pagesCompetency Based Training Programme: DNB-RheumatologyDadNo ratings yet
- 0002 Rheumatology Notes 2015.... 49Document58 pages0002 Rheumatology Notes 2015.... 49Abdul QuyyumNo ratings yet
- Infectious Arthritis: Marshell Tendean, MD Department of Internal Medicine UKRIDA Faculty of Medicine Jakarta IndonesiaDocument56 pagesInfectious Arthritis: Marshell Tendean, MD Department of Internal Medicine UKRIDA Faculty of Medicine Jakarta Indonesiakintan utamiNo ratings yet
- Endocarditis PediatricDocument56 pagesEndocarditis Pediatricfarzzana100% (1)
- Wilson S DiseaseDocument28 pagesWilson S DiseasemichaelcylNo ratings yet
- Rheumatology NotesDocument10 pagesRheumatology NotesBrandonRyanF.MosidinNo ratings yet
- DM CBLDocument18 pagesDM CBLbpt2No ratings yet
- Ankylosing SpondylitisDocument56 pagesAnkylosing Spondylitistitle1989No ratings yet
- Bds Third Professional Examination 2007 General Medicine Table of Specifications Chapter Wise Distribution of Mcqs and SeqsDocument5 pagesBds Third Professional Examination 2007 General Medicine Table of Specifications Chapter Wise Distribution of Mcqs and SeqsJavariya AshrafNo ratings yet
- Transfusion RXNDocument17 pagesTransfusion RXNbeautifulbeastNo ratings yet
- Community RheumatologyDocument8 pagesCommunity Rheumatologyfindingnemo667No ratings yet
- Internal OSCE All Past Years QuestionsDocument17 pagesInternal OSCE All Past Years QuestionsOmar Nayef TaaniNo ratings yet
- Diagnostic Strategy in RheumatologyDocument25 pagesDiagnostic Strategy in Rheumatologyaa031987No ratings yet
- Approach To Arthritis: Clinical GuideDocument4 pagesApproach To Arthritis: Clinical GuideaveekumbharNo ratings yet
- Sameer Smadi MD. Amman-Jordan: Consultant HBP and Liver Transplantation SurgeonDocument179 pagesSameer Smadi MD. Amman-Jordan: Consultant HBP and Liver Transplantation SurgeonNessreen JamalNo ratings yet
- Rheumatology Cases Fall Clinics 2019Document85 pagesRheumatology Cases Fall Clinics 2019NaziBrola TsivadzeNo ratings yet
- Knee Differential DiagnosisDocument2 pagesKnee Differential DiagnosisJade Kenneth Gonzales LomansocNo ratings yet
- Septic ArthritisDocument22 pagesSeptic ArthritisAiman ZakiNo ratings yet
- Pain PowerpointDocument50 pagesPain PowerpointRicardo Pascual100% (1)
- 2021 American College of Rheumatology Vasculitis FoundationDocument10 pages2021 American College of Rheumatology Vasculitis FoundationVerónica Duménez JofréNo ratings yet
- Cranial Nerve ExaminationDocument45 pagesCranial Nerve ExaminationTanat AsavisanuNo ratings yet
- Disorders of Calcium and Phosphate MetabolismDocument20 pagesDisorders of Calcium and Phosphate MetabolismAhmed Noureldin AhmedNo ratings yet
- Seronegative Antiphospholipid SyndromeDocument3 pagesSeronegative Antiphospholipid SyndromealexandruNo ratings yet
- Final Paper 1Document15 pagesFinal Paper 1malaz adil100% (1)
- Transfusion For ChildrenDocument5 pagesTransfusion For ChildrenKristine Mae AbrasaldoNo ratings yet
- HivDocument36 pagesHivfenendriyaniNo ratings yet
- 1a-Introduction To MedicineDocument156 pages1a-Introduction To MedicineEshetu BizunehNo ratings yet
- CBL 101Document446 pagesCBL 101YS NateNo ratings yet
- CBL HypertensionDocument23 pagesCBL HypertensionWan AswanNo ratings yet
- Growth and Development: Infancy Early Childhood Middle Childhood AdolescentDocument47 pagesGrowth and Development: Infancy Early Childhood Middle Childhood AdolescentJamna MaharajNo ratings yet
- ANCA Associated VasculitisDocument62 pagesANCA Associated VasculitispoluashokNo ratings yet
- Hospital VS Form PDFDocument2 pagesHospital VS Form PDFsaguliteNo ratings yet
- Management of Ankylosis Spondylitis 1Document53 pagesManagement of Ankylosis Spondylitis 1ishaan kharbandaNo ratings yet
- TB MeningeDocument75 pagesTB MeningeAyen FornollesNo ratings yet
- Practical Approach To Common Electrolyte EmergenciesDocument64 pagesPractical Approach To Common Electrolyte EmergenciesSamer MatarNo ratings yet
- Septic Arthritis: Pamela Gregory-Fernandez, PA-C SVCMC PA Education ProgramDocument14 pagesSeptic Arthritis: Pamela Gregory-Fernandez, PA-C SVCMC PA Education ProgramtitotamaNo ratings yet
- Vasculitis ReviewDocument128 pagesVasculitis ReviewAjmal RashidNo ratings yet
- Approach To The Patient With Rheumatic DiseaseDocument11 pagesApproach To The Patient With Rheumatic DiseasetedplushNo ratings yet
- Systemic Lupus ErythematosusDocument40 pagesSystemic Lupus ErythematosusAkshan SentinelNo ratings yet
- Helping Baby To BreathDocument49 pagesHelping Baby To BreathmohdmaghyrehNo ratings yet
- RheumatologyDocument55 pagesRheumatologyYeli VeMeNo ratings yet
- Carpel Tunnel SyndromeDocument12 pagesCarpel Tunnel Syndromeyordin deontaNo ratings yet
- Rheumatology PDFDocument80 pagesRheumatology PDFShaheduzzaman LingkonNo ratings yet
- Engine Assembly (3Zz Fe/4Zz Fe) : InspectionDocument4 pagesEngine Assembly (3Zz Fe/4Zz Fe) : Inspectionพลูโตเนียม สองสามเก้าNo ratings yet
- Seizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityDocument50 pagesSeizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityArvindhanNo ratings yet
- Optic Neuritis in Association With Multiple Sclerosis: Hanina Yuthi M 030.09.106Document19 pagesOptic Neuritis in Association With Multiple Sclerosis: Hanina Yuthi M 030.09.106june20000No ratings yet
- Polymyositis DermatomyositisDocument2 pagesPolymyositis DermatomyositisTay Woo ChiaoNo ratings yet
- Rheumatology & Rehabilitation 2018-2019Document57 pagesRheumatology & Rehabilitation 2018-2019Selim TarekNo ratings yet
- Localizing The LesionDocument30 pagesLocalizing The LesionTracy NwanneNo ratings yet
- Systemic Lupus Erythematosus Disease Activity Index SELENA ModificationDocument4 pagesSystemic Lupus Erythematosus Disease Activity Index SELENA ModificationaminahrahimiNo ratings yet
- Diseases of ImmunityDocument55 pagesDiseases of ImmunityMeera ANN AJINo ratings yet
- Nsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyDocument65 pagesNsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyYousef JafarNo ratings yet
- Psoriatic ArthritisDocument4 pagesPsoriatic ArthritisAini Nur Syafa'ahNo ratings yet
- Rheumatoid Arthritis: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 2/ 11/ 2020Document54 pagesRheumatoid Arthritis: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 2/ 11/ 2020Alan K Mhamad100% (1)
- Update in Internal Medicine - 2020: AnnualDocument8 pagesUpdate in Internal Medicine - 2020: AnnualVictor Hugo MartinezNo ratings yet
- Systemic Vasculitis: A Clinical Approach: Geordie Lawry MDDocument65 pagesSystemic Vasculitis: A Clinical Approach: Geordie Lawry MDLydwiNa Jc100% (1)
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Serenity RPG Firefly Role Playing Game PDFDocument225 pagesSerenity RPG Firefly Role Playing Game PDFNathaniel Broyles67% (3)
- Reviewer in EntrepreneurshipDocument6 pagesReviewer in EntrepreneurshipRachelle Anne SaldeNo ratings yet
- Engine Stalls at Low RPM: Diagnostic CodesDocument3 pagesEngine Stalls at Low RPM: Diagnostic CodesAmir Bambang YudhoyonoNo ratings yet
- History of Drilling PDFDocument9 pagesHistory of Drilling PDFNguyen Van TinhNo ratings yet
- DLL in Health 7 3rd QuarterDocument2 pagesDLL in Health 7 3rd QuarterJuna Lyn Hermida ArellonNo ratings yet
- Southern California International Gateway Final Environmental Impact ReportDocument40 pagesSouthern California International Gateway Final Environmental Impact ReportLong Beach PostNo ratings yet
- LMSTC Questionnaire EFFECTIVENESS IN THE IMPLEMENTATION OF LUCENA MANPOWER SKILLS TRAINING CENTER BASIS FOR PROGRAM ENHANCEMENTDocument3 pagesLMSTC Questionnaire EFFECTIVENESS IN THE IMPLEMENTATION OF LUCENA MANPOWER SKILLS TRAINING CENTER BASIS FOR PROGRAM ENHANCEMENTCriselda Cabangon DavidNo ratings yet
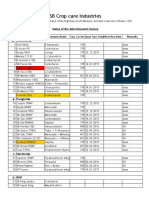
- Products ListDocument11 pagesProducts ListPorag AhmedNo ratings yet
- You're reading a free preview. Pages 4 to 68 are not shown in this preview. Leer la versión completa You're Reading a Free Preview Page 4 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 5 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 6 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 7 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 8 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 9 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 10 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 11 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 12 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 13 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 14 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 15 is notDocument9 pagesYou're reading a free preview. Pages 4 to 68 are not shown in this preview. Leer la versión completa You're Reading a Free Preview Page 4 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 5 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 6 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 7 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 8 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 9 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 10 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 11 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 12 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 13 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 14 is not shown in this preview. DESCARGA You're Reading a Free Preview Page 15 is notFernando ToretoNo ratings yet
- Rolling TechnologyDocument4 pagesRolling TechnologyFrancis Erwin Bernard100% (1)
- Rate If Iodine and PropanoneDocument3 pagesRate If Iodine and Propanoneshareef1No ratings yet
- Influence of Freezing and Pasteurization of The Physical Condition of The Plastik (PE, PP and HDPE) As Selar Fish Packaging (Selaroides Leptolepis) in Sendang Biru, Malang, East Java. IndonesiaDocument7 pagesInfluence of Freezing and Pasteurization of The Physical Condition of The Plastik (PE, PP and HDPE) As Selar Fish Packaging (Selaroides Leptolepis) in Sendang Biru, Malang, East Java. IndonesiaInternational Network For Natural SciencesNo ratings yet
- OnTime Courier Software System Requirements PDFDocument1 pageOnTime Courier Software System Requirements PDFbilalNo ratings yet
- Multibody Dynamics Modeling and System Identification For A Quarter-Car Test Rig With McPherson Strut Suspension PDFDocument122 pagesMultibody Dynamics Modeling and System Identification For A Quarter-Car Test Rig With McPherson Strut Suspension PDFnecromareNo ratings yet
- Coefficient of Restitution - Center of MassDocument3 pagesCoefficient of Restitution - Center of MassMannyCesNo ratings yet
- Pds Hempel's Maestro Water Borne Primer 28830 En-GbDocument2 pagesPds Hempel's Maestro Water Borne Primer 28830 En-GbKalaiyazhagan ElangeeranNo ratings yet
- Mongodb TutorialDocument106 pagesMongodb TutorialRahul VashishthaNo ratings yet
- NATO Obsolescence Management PDFDocument5 pagesNATO Obsolescence Management PDFluisNo ratings yet
- Medical Equipment Quality Assurance For Healthcare FacilitiesDocument5 pagesMedical Equipment Quality Assurance For Healthcare FacilitiesJorge LopezNo ratings yet
- Partnership LiquidationDocument46 pagesPartnership LiquidationSewale Abate79% (19)
- Volvo Catalog Part2Document360 pagesVolvo Catalog Part2Denis Konovalov71% (7)
- Lesson 23 Career PathwaysDocument34 pagesLesson 23 Career PathwaysAlfredo ModestoNo ratings yet
- A Tall Order - Cooling Dubai's Burj Khalifa: FeatureDocument2 pagesA Tall Order - Cooling Dubai's Burj Khalifa: FeatureMohsin KhanNo ratings yet
- Alto Hotel Melbourne GreenDocument2 pagesAlto Hotel Melbourne GreenShubham GuptaNo ratings yet
- Molde Soldadura TADocument1 pageMolde Soldadura TAMarcos Ivan Ramirez AvenaNo ratings yet
- Operator'S Manual PM20X-X-X-BXX: 2" Diaphragm PumpDocument12 pagesOperator'S Manual PM20X-X-X-BXX: 2" Diaphragm PumpOmar TadeoNo ratings yet
- ABHIGYAN 2020 E-InvitationDocument2 pagesABHIGYAN 2020 E-Invitationchirag sabhayaNo ratings yet
- Ziarek - The Force of ArtDocument233 pagesZiarek - The Force of ArtVero MenaNo ratings yet
- IFSSO Newsletter Jul-Sep 2010Document2 pagesIFSSO Newsletter Jul-Sep 2010rjotaduranNo ratings yet
- The Chulalongkorn Centenary ParkDocument6 pagesThe Chulalongkorn Centenary ParkJack FooNo ratings yet