You might also like
- Nursing the NeonateFrom EverandNursing the NeonateMaggie MeeksNo ratings yet
- Immediate Newborn Care Updates at San Isidro CollegeDocument11 pagesImmediate Newborn Care Updates at San Isidro CollegeMay Princes Torregosa Abucejo100% (1)
- Immediate Care of The NewbornDocument11 pagesImmediate Care of The NewbornHannahKarizaNo ratings yet
- Essential Newborn Care GuideDocument120 pagesEssential Newborn Care Guidejuly3ciaNo ratings yet
- Newborn Screening 1Document47 pagesNewborn Screening 1Jhon Lapuz100% (1)
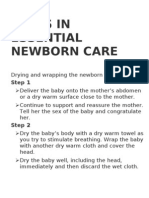
- Steps in Essential Newborn CareDocument12 pagesSteps in Essential Newborn CareCedy L. CieloNo ratings yet
- Nursing Care of At-Risk NewbornsDocument256 pagesNursing Care of At-Risk NewbornsAaron ConstantinoNo ratings yet
- Baby Friendly Hospital Initiative (Bfhi)Document9 pagesBaby Friendly Hospital Initiative (Bfhi)Ankita BramheNo ratings yet
- Prenatal Care Importance and ScheduleDocument23 pagesPrenatal Care Importance and ScheduleMaxinne Allyssa Cancino RoseñoNo ratings yet
- Health assessment ADPIE nursing processDocument2 pagesHealth assessment ADPIE nursing processKrishna Faith P. DelaraNo ratings yet
- Severe Acute MalnutritionDocument4 pagesSevere Acute MalnutritionAlemayehu DargeNo ratings yet
- H EducDocument82 pagesH EducJennifer Solano CruelNo ratings yet
- 10 Steps To Successful Breastfeeding 2Document39 pages10 Steps To Successful Breastfeeding 2Quennie Marie Moreno VillanuevaNo ratings yet
- Einc Eval ExamDocument8 pagesEinc Eval ExamMaxeneDhaleNo ratings yet
- Integrated Management of Childhood IllnessDocument195 pagesIntegrated Management of Childhood Illnesskarendelarosa06277100% (1)
- Essential Intrapartum Newborn Care 181120082158 PDFDocument19 pagesEssential Intrapartum Newborn Care 181120082158 PDFDorinna Rizada BagaNo ratings yet
- Apgar ScoreDocument11 pagesApgar Scorefaizura100% (1)
- Expanded Program On Immunization: University of The Philippines ManilaDocument39 pagesExpanded Program On Immunization: University of The Philippines ManilaNik Rose ElNo ratings yet
- DOH Maternal Health ProgramDocument5 pagesDOH Maternal Health ProgramErwin Jake TagubaNo ratings yet
- Maternal & Child NUrsing SylabusDocument7 pagesMaternal & Child NUrsing Sylabusmarsan12No ratings yet
- Applying Restraint Nursing SkillDocument2 pagesApplying Restraint Nursing SkillEiichiro BertoNo ratings yet
- IMCI Session 3-The Integrated Case Management ProcessDocument67 pagesIMCI Session 3-The Integrated Case Management Processsarguss1480% (5)
- Newborn Mentoring Checklist, Feb 13, 2020Document14 pagesNewborn Mentoring Checklist, Feb 13, 2020AlemsegedNo ratings yet
- Assessing High Risk NewbornsDocument42 pagesAssessing High Risk NewbornsKiran KumarNo ratings yet
- Achieving Newborn Care CompetencyDocument2 pagesAchieving Newborn Care CompetencyShekaina BartidoNo ratings yet
- The Intrauterine Device: HealthDocument2 pagesThe Intrauterine Device: HealthApris Tesryanto LiufetoNo ratings yet
- Nursing Care For NewbornDocument33 pagesNursing Care For NewbornDarla Quiballo100% (1)
- 3 - High Risk InfantDocument30 pages3 - High Risk InfantMohammed AtaNo ratings yet
- WHO - IMCI-Integrated Management of Childhood IllnessDocument60 pagesWHO - IMCI-Integrated Management of Childhood Illnesseric100% (1)
- 1 - EINC With InstrumentationDocument39 pages1 - EINC With InstrumentationDaenna Corrine JerezaNo ratings yet
- Case Scenario #4 (Postpartum)Document3 pagesCase Scenario #4 (Postpartum)Krizzia Angela BacotocNo ratings yet
- Prematurity and PostmaturityDocument34 pagesPrematurity and PostmaturityAngelo MolinaNo ratings yet
- Nursing Bullets: Fundamentals of Nursing ReviewerDocument44 pagesNursing Bullets: Fundamentals of Nursing ReviewerErl DiamanteNo ratings yet
- MCN Lab WRDocument101 pagesMCN Lab WRMaui TabuzoNo ratings yet
- High Risk NewbornDocument24 pagesHigh Risk NewbornYemaya84No ratings yet
- Essential Intrapartum and Newborn CareDocument160 pagesEssential Intrapartum and Newborn CareJohn Alwyn Hernandez100% (1)
- Complimentory Feeding 2Document10 pagesComplimentory Feeding 2Silji AntonyNo ratings yet
- Resuscitation of New Born: SBA - Presentation 5 (B)Document27 pagesResuscitation of New Born: SBA - Presentation 5 (B)Dr-Nikhil Goswami100% (1)
- Maternal & Child Nursing Care: Lecture NotesDocument42 pagesMaternal & Child Nursing Care: Lecture NotesMidori San100% (1)
- Medical Colleges of Northern PhilippinesDocument2 pagesMedical Colleges of Northern PhilippinesAmiel Francisco Reyes100% (3)
- Nursing Practice I - Foundation of Professional Nursing Practice - RNpediaDocument2 pagesNursing Practice I - Foundation of Professional Nursing Practice - RNpediaBrianMarBeltranNo ratings yet
- Instructional PlanDocument6 pagesInstructional PlanJuriel Michael Alap100% (1)
- Family PlanningDocument13 pagesFamily PlanningYana PotNo ratings yet
- Neonatal SepsisDocument22 pagesNeonatal Sepsisjake1014100% (1)
- Assessment in PregnancyDocument34 pagesAssessment in PregnancyPatricia Anne Nicole CuaresmaNo ratings yet
- Essential Newborn CareDocument104 pagesEssential Newborn CareRaidis PangilinanNo ratings yet
- Breastfeeding TPDocument3 pagesBreastfeeding TPAndrea Mae SanchezNo ratings yet
- Pediatric Dehydration: A Guide to Assessment and ManagementDocument14 pagesPediatric Dehydration: A Guide to Assessment and ManagementReimer LaquihuanacoNo ratings yet
- Integrated Management of Childhood IllnessDocument52 pagesIntegrated Management of Childhood IllnessRitz CelsoNo ratings yet
- Newborn Screening ImportanceDocument7 pagesNewborn Screening ImportanceSeph LiwanagNo ratings yet
- 10 Steps Successful BreastfeedingDocument66 pages10 Steps Successful BreastfeedingFayrouz EssawiNo ratings yet
- COVID-19: Knowledge Base, Attitudes and Practices Among Practising Journalists in Abuja, NigeriaDocument13 pagesCOVID-19: Knowledge Base, Attitudes and Practices Among Practising Journalists in Abuja, NigeriaPremier PublishersNo ratings yet
- Care of The Woman During PregnancyDocument99 pagesCare of The Woman During PregnancyFrancr ToledanoNo ratings yet
- IMCIDocument112 pagesIMCIJohann Dexter Malimban GloriosoNo ratings yet
- Mother Friendly Care PracticesDocument67 pagesMother Friendly Care PracticesSeth Josiah E. MacalaladNo ratings yet
- Essential Intrapartum and Newborn CareDocument37 pagesEssential Intrapartum and Newborn CareVenice s SantosNo ratings yet
- Newborn CareDocument120 pagesNewborn CareMike CalipayanNo ratings yet
- Physiologic Assessment of Newborn, Newborn Adaptation and Normal Growth & DevelopmentDocument4 pagesPhysiologic Assessment of Newborn, Newborn Adaptation and Normal Growth & DevelopmentBernard M. Lapuz FullNo ratings yet
- Newborn Care StepsDocument58 pagesNewborn Care StepsMerlin AshlyNo ratings yet
- New Born ResuscitationDocument49 pagesNew Born ResuscitationdivyamuthyalaNo ratings yet
- Form TQF.3 English B.A.Document13 pagesForm TQF.3 English B.A.Hurley ReefNo ratings yet
- Fundamentals of Nursing Therapeutics Evaluation Form For Student Nurse's Character Fundamentals of Nursing A FinalDocument1 pageFundamentals of Nursing Therapeutics Evaluation Form For Student Nurse's Character Fundamentals of Nursing A FinalHurley ReefNo ratings yet
- 4 Laboratory GuidelinesDocument1 page4 Laboratory GuidelinesHurley ReefNo ratings yet
- The Importance of ExerciseDocument43 pagesThe Importance of ExerciseHurley ReefNo ratings yet
- Application Letter (NSO, DSWD)Document1 pageApplication Letter (NSO, DSWD)Hurley Reef82% (67)
- Heat ColdDocument15 pagesHeat ColdHurley ReefNo ratings yet
- Laboratory RequestDocument1 pageLaboratory RequestHurley ReefNo ratings yet
- Form: FM Course Specifications (TQF. 3) : Code: FM-ACS-004.02 Issued: 3 October 2012 Revised No. 2Document2 pagesForm: FM Course Specifications (TQF. 3) : Code: FM-ACS-004.02 Issued: 3 October 2012 Revised No. 2Hurley ReefNo ratings yet
- Wathuaichorakhie Wittayakhom School: WorksheetDocument1 pageWathuaichorakhie Wittayakhom School: Worksheetgladz25No ratings yet
- ENGLISH V Single PassageDocument12 pagesENGLISH V Single PassageHurley ReefNo ratings yet
- Endocrine 2Document10 pagesEndocrine 2Hurley ReefNo ratings yet
- Hospital AdmissionDocument27 pagesHospital AdmissionHurley ReefNo ratings yet
- Ihum 3010 TQF 3Document12 pagesIhum 3010 TQF 3Hurley ReefNo ratings yet
- Syllabus - Theory and PracticeDocument5 pagesSyllabus - Theory and PracticeHurley ReefNo ratings yet
- ENGLISH V Single PassageDocument12 pagesENGLISH V Single PassageHurley ReefNo ratings yet
- Maternal and Child NursingDocument23 pagesMaternal and Child Nursingdesh08No ratings yet
- Assessment - Nursing Care PlanDocument2 pagesAssessment - Nursing Care PlanHurley ReefNo ratings yet
- Integumentary SystemDocument102 pagesIntegumentary SystemHurley ReefNo ratings yet
- Identify The Indicated Structures On This Eukaryotic Cell2Document2 pagesIdentify The Indicated Structures On This Eukaryotic Cell2Hurley ReefNo ratings yet
- Sample Format Invitation LetterDocument3 pagesSample Format Invitation LetterHurley Reef100% (9)
- A Brief History of PharmacologyDocument3 pagesA Brief History of PharmacologyHurley Reef100% (1)
- Rle Grading SystemDocument5 pagesRle Grading SystemHurley ReefNo ratings yet
- Evaluation ToolDocument8 pagesEvaluation ToolHurley ReefNo ratings yet
- PercocetDocument2 pagesPercocetNinoska Garcia-OrtizNo ratings yet
- AIAPGET 2018 analysisDocument4 pagesAIAPGET 2018 analysisarpit sachanNo ratings yet
- Giacomo Zaccone-Fish Defenses Vol. 1 Immunology (Teleostean Fish Biology A Com) - 1-Science Publishers (2009)Document379 pagesGiacomo Zaccone-Fish Defenses Vol. 1 Immunology (Teleostean Fish Biology A Com) - 1-Science Publishers (2009)Beatrice SavaNo ratings yet
- Type III ReactionsDocument2 pagesType III ReactionsRch 19No ratings yet
- ECSI Instructor Update 2021Document52 pagesECSI Instructor Update 2021Zach MatthewsNo ratings yet
- Indriatmi, W. 2018. Ilmu Penyakit Dan Kulit Kelamin. Edisi Ke-7. Jakarta: Badan Penerbit Fakultas Kedokteran IndonesiaDocument10 pagesIndriatmi, W. 2018. Ilmu Penyakit Dan Kulit Kelamin. Edisi Ke-7. Jakarta: Badan Penerbit Fakultas Kedokteran IndonesiaDiza Hanni PertiwiNo ratings yet
- Herpes Simplex I and IIDocument50 pagesHerpes Simplex I and IItummalapalli venkateswara raoNo ratings yet
- 01 MynckeDocument10 pages01 MynckeIrina DesyatykhNo ratings yet
- Hesi Med Surg-14Document1 pageHesi Med Surg-14GeorgeNo ratings yet
- Overview of Digestive System 16-01-23Document20 pagesOverview of Digestive System 16-01-23erisericssonNo ratings yet
- Toxic Megacolon: Daniel M. Autenrieth, MD, and Daniel C. Baumgart, MD, PHDDocument8 pagesToxic Megacolon: Daniel M. Autenrieth, MD, and Daniel C. Baumgart, MD, PHDGoran TomićNo ratings yet
- JevaxDocument2 pagesJevaxjovedNo ratings yet
- Gulan 2003 Klinicka - I - Radioloska - Prezentacija - Kostanih Medri - 1319 Publishedversion H0k4iq SDocument10 pagesGulan 2003 Klinicka - I - Radioloska - Prezentacija - Kostanih Medri - 1319 Publishedversion H0k4iq SMuxoliniNo ratings yet
- Boot CampDocument190 pagesBoot CampfekaduNo ratings yet
- Risk Assessment Chart - WaterlowDocument2 pagesRisk Assessment Chart - WaterlowRalucaNo ratings yet
- ITLS 8e Advanced Post Test Exam Version BDocument10 pagesITLS 8e Advanced Post Test Exam Version BMohamed TabanaNo ratings yet
- TETRASODIUM EDTA - National Library of Medicine HSDB DatabaseDocument21 pagesTETRASODIUM EDTA - National Library of Medicine HSDB DatabaseElena TrofinNo ratings yet
- Immediate Post-Anaesthesia Recovery 2013Document20 pagesImmediate Post-Anaesthesia Recovery 2013gythrieNo ratings yet
- Calorimetría Indirecta EsencialDocument12 pagesCalorimetría Indirecta EsencialPaulina ToledoNo ratings yet
- L ArginineDocument3 pagesL ArginineZioAngelNo ratings yet
- MdsDocument570 pagesMdsAgus SusantoNo ratings yet
- Indisposition & Their CauseDocument13 pagesIndisposition & Their Causenaazsaheba448No ratings yet
- Fluid and Electrolyte Nursing Care Management 112Document7 pagesFluid and Electrolyte Nursing Care Management 112anne marieNo ratings yet
- Treatment Plan TemplatesDocument2 pagesTreatment Plan TemplatesShalini Dass100% (3)
- MCQ MedicineDocument4 pagesMCQ MedicineKasun PereraNo ratings yet
- Study On Effect of Wet Cupping (Hijama) On Blood Lipid Profile in Human at Aldyssah-Alshati, LibyaDocument4 pagesStudy On Effect of Wet Cupping (Hijama) On Blood Lipid Profile in Human at Aldyssah-Alshati, LibyaMohammed Ramzy GhifariNo ratings yet
- Mrcem Primary June 2022 Recalls Compiled by DR Sumair HameedDocument4 pagesMrcem Primary June 2022 Recalls Compiled by DR Sumair HameedSHK100% (1)
- Disease Research PaperDocument6 pagesDisease Research PaperJose PalaciosNo ratings yet
- Stem Cell Therapy and EthicsDocument2 pagesStem Cell Therapy and EthicsRaniya Khan [Student]No ratings yet
- Chapter 35: Eye Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument5 pagesChapter 35: Eye Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet