You might also like
- Science Workbook 2ndDocument83 pagesScience Workbook 2ndluluNo ratings yet
- Joint Replacement Anesthesia ManagementDocument55 pagesJoint Replacement Anesthesia ManagementRaguNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Failed Spinal AnaesthesiaDocument10 pagesFailed Spinal Anaesthesian12345678n100% (1)
- CH 46 Complications of AnaesthesiaDocument29 pagesCH 46 Complications of AnaesthesiaChristian LeepoNo ratings yet
- 3.preoperative Patient Assessment and ManagementDocument76 pages3.preoperative Patient Assessment and Managementoliyad alemayehuNo ratings yet
- Epidural AnesthesiaDocument5 pagesEpidural AnesthesiaImran MukhlessNo ratings yet
- ICSE Solutions For Class 10 Biology - The Excretory System - A Plus TopperDocument28 pagesICSE Solutions For Class 10 Biology - The Excretory System - A Plus TopperSuresh Kumar100% (1)
- Anesthesia: Mrs - SanthiDocument59 pagesAnesthesia: Mrs - SanthisanthiyasandyNo ratings yet
- Preoperative Patient Assessment and Management: Roxanne Jeen L. FornollesDocument61 pagesPreoperative Patient Assessment and Management: Roxanne Jeen L. FornollesRyan FornollesNo ratings yet
- Managing Difficult Airway in Obstetric AnesthesiaDocument3 pagesManaging Difficult Airway in Obstetric AnesthesiaRoman AureliaNo ratings yet
- Anesthesia For ElderlyDocument27 pagesAnesthesia For ElderlyApril Joy CalayagNo ratings yet
- Anesthesia For Bariatric SurgeryDocument47 pagesAnesthesia For Bariatric Surgerydkhiloi100% (1)
- AnaesthesiaDocument121 pagesAnaesthesiaSandeep Bhangale100% (1)
- Anesthesia For Robotic Surgery - FinalDocument21 pagesAnesthesia For Robotic Surgery - FinalDr. Sunila SharmaNo ratings yet
- Fred Rotenberg, MD Dept. of Anesthesiology Rhode Island Hospital Grand Rounds February 27, 2008Document53 pagesFred Rotenberg, MD Dept. of Anesthesiology Rhode Island Hospital Grand Rounds February 27, 2008lmjeksoreNo ratings yet
- Anaesthetic Management in Laparoscopic SurgeriesDocument39 pagesAnaesthetic Management in Laparoscopic SurgeriesRaguNo ratings yet
- Complications of Spinal and Epidural AnesthesiaDocument45 pagesComplications of Spinal and Epidural AnesthesiashikhaNo ratings yet
- Important CPSP Points 2015-2016Document91 pagesImportant CPSP Points 2015-2016naeem2009100% (2)
- Anesthesia For Genitourinary SurgeryDocument76 pagesAnesthesia For Genitourinary SurgeryWenny Eka FildayantiNo ratings yet
- Anaesthesia in Obese PatientsDocument72 pagesAnaesthesia in Obese PatientsPraveen RamasamyNo ratings yet
- Uro-Radiology Text and AtlassDocument257 pagesUro-Radiology Text and Atlassnancymariscal100% (1)
- Management of Kidney Diseases 2023Document579 pagesManagement of Kidney Diseases 2023Mauricio LopezNo ratings yet
- Epidural Anatomy & PhysiologyDocument14 pagesEpidural Anatomy & PhysiologyAbel AxelNo ratings yet
- Thoraxic Region Nerve Block - ESADocument35 pagesThoraxic Region Nerve Block - ESAMaraNo ratings yet
- Anesthesia for thyroid disease or surgeryDocument12 pagesAnesthesia for thyroid disease or surgeryJavier GlezqNo ratings yet
- NMJ Blocking Agents GuideDocument69 pagesNMJ Blocking Agents Guidevvb_frndNo ratings yet
- Controlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewDocument49 pagesControlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewAnn Susan MathewNo ratings yet
- Airway Management Inside and Outside Operating Rooms 2018 British Journal ofDocument3 pagesAirway Management Inside and Outside Operating Rooms 2018 British Journal ofSeveNNo ratings yet
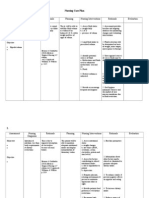
- Nursing Care Plan CKDDocument6 pagesNursing Care Plan CKDReylan Deo Rallo Asio100% (5)
- ANESTHESIA-Pediatrics Airway SyndromesDocument12 pagesANESTHESIA-Pediatrics Airway SyndromeshollyuNo ratings yet
- 21 Obstetric Anaesthesia PDFDocument0 pages21 Obstetric Anaesthesia PDFjuniorebindaNo ratings yet
- Obesity & Anaesthesia: Co-Ordinator - Dr. Chavi Sethi (MD) Speaker - Dr. Uday Pratap SinghDocument56 pagesObesity & Anaesthesia: Co-Ordinator - Dr. Chavi Sethi (MD) Speaker - Dr. Uday Pratap SinghRafi ramdhanNo ratings yet
- Anesthesia For Robotic Surgery - FinalDocument21 pagesAnesthesia For Robotic Surgery - FinalDr. Sunila SharmaNo ratings yet
- Pediatric Anesthesiology Review: Clinical Cases for Self-AssessmentFrom EverandPediatric Anesthesiology Review: Clinical Cases for Self-AssessmentNo ratings yet
- DVT ProphylaxisDocument30 pagesDVT ProphylaxissivaNo ratings yet
- Preanesthetic Medication JasminaDocument44 pagesPreanesthetic Medication Jasminaanjali sNo ratings yet
- Brachial Plexus Block TechniquesDocument13 pagesBrachial Plexus Block TechniquesAnkit Shah100% (1)
- Cardio-Hepatology: Connections Between Hepatic and Cardiovascular DiseaseFrom EverandCardio-Hepatology: Connections Between Hepatic and Cardiovascular DiseaseTatsunori TaniguchiNo ratings yet
- Anaesthesia For Neuroradiological Procedures Premalatha SDocument48 pagesAnaesthesia For Neuroradiological Procedures Premalatha SPrema LathaNo ratings yet
- Anesthesia Considerations For Neuromuscular DiseaseDocument42 pagesAnesthesia Considerations For Neuromuscular Diseasesamrox54No ratings yet
- Co-Ordinated By: DR Parul Presented By: DR GurneetDocument45 pagesCo-Ordinated By: DR Parul Presented By: DR Gurneetreenujohney100% (2)
- Medical and Surgical NursingDocument4 pagesMedical and Surgical NursingCrystal Ann Monsale TadiamonNo ratings yet
- 4.muscle RelaxantsDocument23 pages4.muscle Relaxantskarim hassanNo ratings yet
- Anaesthesia in Liver Disease PatientDocument49 pagesAnaesthesia in Liver Disease PatientVG FernandezNo ratings yet
- Patient Monitoring1370Document53 pagesPatient Monitoring1370Ridha Surya NugrahaNo ratings yet
- Management of Intraoperative Bronchospasm: Dr. ImranDocument49 pagesManagement of Intraoperative Bronchospasm: Dr. ImranhellodrvigneshwarNo ratings yet
- Difficult Airway Management TechniquesDocument54 pagesDifficult Airway Management TechniquesAnonymous V5xDcrNo ratings yet
- Controlled Hypotensive AnesthesiaDocument24 pagesControlled Hypotensive AnesthesiaSuresh Kumar100% (1)
- One Lung Ventilation: Llalando L. Austin Ii, MHSC, Aa-C, RRT Nova Southeastern UniversityDocument47 pagesOne Lung Ventilation: Llalando L. Austin Ii, MHSC, Aa-C, RRT Nova Southeastern UniversityZulkarnainBustamam100% (1)
- Anesthesia For Kidney TransplantDocument6 pagesAnesthesia For Kidney TransplantachyutsharmaNo ratings yet
- HYPOTHERMIA AND TEMPERATURE REGULATION DURING ANESTHESIADocument20 pagesHYPOTHERMIA AND TEMPERATURE REGULATION DURING ANESTHESIAAgung Bhaktiyar100% (1)
- Failed Spinal Anaesthesia Mechanisms, Management and PreventionDocument6 pagesFailed Spinal Anaesthesia Mechanisms, Management and Preventiondrhemantt1279No ratings yet
- Anesthesia For GeriatricDocument21 pagesAnesthesia For GeriatricintanNo ratings yet
- Pregnancy & Its Anaesthetic ImplicationsDocument29 pagesPregnancy & Its Anaesthetic ImplicationsDadik WijayaNo ratings yet
- Paediatric Anaesthesia PDFDocument33 pagesPaediatric Anaesthesia PDFMarcelitaTaliaDuwiriNo ratings yet
- Factors Affectin Block HeightDocument37 pagesFactors Affectin Block HeightshikhaNo ratings yet
- Anesthesia - State of Narcosis, Analgesia, Relaxation, and Loss of Reflex. Effects of AnesthesiaDocument3 pagesAnesthesia - State of Narcosis, Analgesia, Relaxation, and Loss of Reflex. Effects of AnesthesiaJhevilin RMNo ratings yet
- ADH - Review Low Flow AnesthesiaDocument52 pagesADH - Review Low Flow AnesthesiaAria AdhiatmaNo ratings yet
- Technique For Awake Fibre Optic IntubationDocument3 pagesTechnique For Awake Fibre Optic Intubationmonir61No ratings yet
- Anasthesia in Obese PatientDocument4 pagesAnasthesia in Obese PatientWaNda GrNo ratings yet
- Anaesthesia For Thyroid Surgery....Document46 pagesAnaesthesia For Thyroid Surgery....Parvathy R NairNo ratings yet
- Premedication: by Alif Moderator: Dr. JasmineDocument45 pagesPremedication: by Alif Moderator: Dr. JasmineAlef AminNo ratings yet
- Modern Anaesthesia Machines: Upgrading and SafetyDocument24 pagesModern Anaesthesia Machines: Upgrading and SafetyShiva Kumar P SNo ratings yet
- Essential Concepts for Airway ManagementDocument42 pagesEssential Concepts for Airway Managementkader abdiNo ratings yet
- Spinal Anaesthesia A Practical GuideDocument14 pagesSpinal Anaesthesia A Practical GuideNovita WulandariNo ratings yet
- Intravenous Regonal Anaesthesia Biers BlockDocument2 pagesIntravenous Regonal Anaesthesia Biers BlockOkenabirhieNo ratings yet
- Intraoperative Blood Glucose Levels in Nondiabetic Patients Undergoing Elective Major Surgery Under General Anaesthesia Receiving Different Crystalloid Solutions For Maintenance FluidDocument7 pagesIntraoperative Blood Glucose Levels in Nondiabetic Patients Undergoing Elective Major Surgery Under General Anaesthesia Receiving Different Crystalloid Solutions For Maintenance FluidSouvik MaitraNo ratings yet
- British Consensus Guidelines On Intravenous Fluid Therapy For Adult Surgical Patients Giftasup 2008Document50 pagesBritish Consensus Guidelines On Intravenous Fluid Therapy For Adult Surgical Patients Giftasup 2008Souvik MaitraNo ratings yet
- Can't Intubate - RSIDocument1 pageCan't Intubate - RSIMohammed AhmedNo ratings yet
- Anaesthesia For Renal TransplantationDocument66 pagesAnaesthesia For Renal TransplantationSouvik MaitraNo ratings yet
- Nephrotic vs Nephritic SyndromesDocument3 pagesNephrotic vs Nephritic Syndromeskvs gouthamNo ratings yet
- AsphyxiaDocument48 pagesAsphyxiapavi7muruganathanNo ratings yet
- Material On PHYSIOLOGICAL CHANGES DURING PREGNANCYDocument21 pagesMaterial On PHYSIOLOGICAL CHANGES DURING PREGNANCYAnuradha MauryaNo ratings yet
- MCQ FMS 3 (2016) With Answers-1Document17 pagesMCQ FMS 3 (2016) With Answers-1stella pangestikaNo ratings yet
- Red Urine: Basic (Routine) UrinalysisDocument4 pagesRed Urine: Basic (Routine) UrinalysisMonica DomingoNo ratings yet
- Kadek Miantari (C1118051) Tugas Keperawatan Medikal Bedah IIDocument34 pagesKadek Miantari (C1118051) Tugas Keperawatan Medikal Bedah IIAA Made Agus Dwi SuprasthaNo ratings yet
- Renal Physiology PhysioExDocument30 pagesRenal Physiology PhysioExKim RamosNo ratings yet
- Special Considerations in IV TherapyDocument19 pagesSpecial Considerations in IV TherapyThad AlstrupNo ratings yet
- Urinary System 1. List The Functions of The KidneysDocument6 pagesUrinary System 1. List The Functions of The KidneysheerNo ratings yet
- Interstitial NephritisDocument21 pagesInterstitial NephritisAhmed RaadNo ratings yet
- Acute Kidney Injury and Chronic Kidney DiseaseDocument44 pagesAcute Kidney Injury and Chronic Kidney DiseaseshihochanNo ratings yet
- Chronic Kidney DiseaseDocument3 pagesChronic Kidney DiseaseKinanti Mahmud PraditaNo ratings yet
- CKD EsrdDocument83 pagesCKD EsrdRita Lakhani100% (1)
- Edexcel IGCSE Checklist Biology 9 1Document17 pagesEdexcel IGCSE Checklist Biology 9 1rehan.akaayubNo ratings yet
- KDIGO GN GuidelineDocument143 pagesKDIGO GN GuidelineSamuel Rudolf Maranatha JulioNo ratings yet
- Chronic Kidney Disease Prediction Using Machine LearningDocument7 pagesChronic Kidney Disease Prediction Using Machine Learningy broNo ratings yet
- Cardiorenal SyndromeDocument21 pagesCardiorenal SyndromeAndy McCulloughNo ratings yet
- Kuliah Patologi Klinik FK Undana: Patogenesis Gangguan Substansi Dan Cairan TubuhDocument153 pagesKuliah Patologi Klinik FK Undana: Patogenesis Gangguan Substansi Dan Cairan TubuhtharaNo ratings yet
- WHO News Letter CKDu - A New Threat To HealthDocument2 pagesWHO News Letter CKDu - A New Threat To Healthsandaru86No ratings yet
- Kool Medic Golden 2Document406 pagesKool Medic Golden 2DijattxNo ratings yet
- Activity 2 Urine Types Collection and ProceduresDocument11 pagesActivity 2 Urine Types Collection and ProceduresGlydenne Glaire Poncardas GayamNo ratings yet
- Nephrotic Syndrome (Nephrosis)Document9 pagesNephrotic Syndrome (Nephrosis)Madhusmita SatapathyNo ratings yet
- Anatomy and PhysiologyDocument3 pagesAnatomy and PhysiologyMarielle Leyva AycaydeNo ratings yet