You might also like
- Medication and Health Teaching Discharge PlanDocument1 pageMedication and Health Teaching Discharge PlanBernalene SyNo ratings yet
- NCP 1 Nursing DiagnosisDocument6 pagesNCP 1 Nursing DiagnosisJosh BlasNo ratings yet
- Breast Cancer Detection: Course Task: WEEK 15Document6 pagesBreast Cancer Detection: Course Task: WEEK 15Bunnie AlphaNo ratings yet
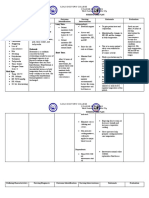
- I. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationDocument4 pagesI. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationCherubim Lei DC FloresNo ratings yet
- NCP ModsDocument5 pagesNCP ModsKirstin del CarmenNo ratings yet
- COURSE TASK 1 Increased ICP POLICIOS, SHARMAINE ANNE M. BSN 3Y2 - 3ADocument2 pagesCOURSE TASK 1 Increased ICP POLICIOS, SHARMAINE ANNE M. BSN 3Y2 - 3ASHARMAINE ANNE POLICIOS100% (1)
- Acute Pain AGEDocument2 pagesAcute Pain AGEHarris AustriaNo ratings yet
- Psychiatric Nursing Pnle 2022Document25 pagesPsychiatric Nursing Pnle 2022Bariwan FaredaNo ratings yet
- FractureDocument4 pagesFractureRaveen mayiNo ratings yet
- Lantus (Insulin Pen) Uses, Dosage, Side Effects - DrugsDocument5 pagesLantus (Insulin Pen) Uses, Dosage, Side Effects - Drugsremyde07No ratings yet
- Ra 11036Document1 pageRa 11036Kiana AbellaNo ratings yet
- Teaching PlanDocument3 pagesTeaching PlanGeralyn KaeNo ratings yet
- Chromium Picolinate Drug StudyDocument1 pageChromium Picolinate Drug StudyjoellaNo ratings yet
- Novilyn C. Pataray Bsn-Ii Retinophathy: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray Bsn-Ii Retinophathy: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- Nursing Process in Drug TherapyDocument32 pagesNursing Process in Drug TherapyChaseNo ratings yet
- Clinical Reasoning Questions - Lupus and Blood DonationDocument4 pagesClinical Reasoning Questions - Lupus and Blood DonationMohammad OmarNo ratings yet
- Metabolism Case StudiesDocument3 pagesMetabolism Case StudiesEpoy Bantawig0% (1)
- Republic ActDocument36 pagesRepublic ActjanNo ratings yet
- Nursing Care Plan For Type1 DiabetesDocument1 pageNursing Care Plan For Type1 DiabetesBushra AlkhdourNo ratings yet
- Essay About DiabetesDocument3 pagesEssay About DiabetesKin Demotica100% (1)
- Monsalud - Drug StudyDocument5 pagesMonsalud - Drug StudyJanielle Christine MonsaludNo ratings yet
- Jane's hospice care focused on pain control and comfortDocument2 pagesJane's hospice care focused on pain control and comfortJackRolunaBernalesNo ratings yet
- University of Northern PhilippinesDocument1 pageUniversity of Northern PhilippinesCezanne CruzNo ratings yet
- Involving Family, Domestic Relations, Women and Children. (2015) - Philippine JudicialDocument10 pagesInvolving Family, Domestic Relations, Women and Children. (2015) - Philippine JudicialAngel MayNo ratings yet
- Prostate Cancer CaseDocument32 pagesProstate Cancer CaseEbere EnyinnaNo ratings yet
- Psychopathology of DepressionDocument3 pagesPsychopathology of DepressionAnanyaNo ratings yet
- Micronutrients and Pregnancy Outcome ReviewDocument1 pageMicronutrients and Pregnancy Outcome ReviewDenisse Shazz Mae MaretNo ratings yet
- 10 Rights of Drug AdministrationDocument1 page10 Rights of Drug AdministrationDoyTanNo ratings yet
- Risk For Bleeding - Cirrhosis NCPDocument2 pagesRisk For Bleeding - Cirrhosis NCPPaula AbadNo ratings yet
- Larcade Arcana LT 2.2 Module 2 The Development of World PoliticsDocument1 pageLarcade Arcana LT 2.2 Module 2 The Development of World PoliticsLarcade ArcanaNo ratings yet
- Clinical ScenarioDocument3 pagesClinical ScenarioGiselle EstoquiaNo ratings yet
- Self-awareness checklist for BSN-3C studentDocument9 pagesSelf-awareness checklist for BSN-3C studentrodamel gundanNo ratings yet
- Significant Dates in the Development of Public Health Nursing in the PhilippinesDocument5 pagesSignificant Dates in the Development of Public Health Nursing in the PhilippinesJenylbajado28No ratings yet
- Subjective: No Subjective Cues. ObjectiveDocument2 pagesSubjective: No Subjective Cues. Objective1S VILLEGAS GabrielNo ratings yet
- Case Study on Graded Return to Work Program for Carpal Tunnel SyndromeDocument11 pagesCase Study on Graded Return to Work Program for Carpal Tunnel SyndromeMargeaux Deb Bartholomew CarleNo ratings yet
- NCPDocument2 pagesNCPTin TinNo ratings yet
- Health Teaching Plan ContentDocument2 pagesHealth Teaching Plan ContentEdmr Slzar100% (1)
- Imbalanced NutritionDocument2 pagesImbalanced NutritionRizza 이 동해 Ocampo100% (1)
- Which It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToDocument8 pagesWhich It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToAriane-Gay Cristobal DuranNo ratings yet
- NCP and Drug StudyDocument5 pagesNCP and Drug StudyVincent Maralit MaterialNo ratings yet
- Ra 10344Document6 pagesRa 10344Lrac KangNo ratings yet
- NURSING CARE PLAN FOR RHEUMATIC HEART DISEASEDocument11 pagesNURSING CARE PLAN FOR RHEUMATIC HEART DISEASECharm TanyaNo ratings yet
- NCP Liver CirrhosisDocument5 pagesNCP Liver CirrhosisEsther O. CorreaNo ratings yet
- VM211 MODULE 5 Developing Ethics2Document2 pagesVM211 MODULE 5 Developing Ethics2tonizia lopezNo ratings yet
- Jacildo LT Module 6 TCNDocument2 pagesJacildo LT Module 6 TCNMeryville JacildoNo ratings yet
- Week - 7 Rle 312Document5 pagesWeek - 7 Rle 312VAL ASHLIE ACEBARNo ratings yet
- NCPDocument9 pagesNCPLeolene Grace BautistaNo ratings yet
- NCP T2DMDocument5 pagesNCP T2DMFrancym R. BatengaNo ratings yet
- Topic 1: Introduction To Geria Nursing: Activity 1.1: Grandparents' LoveDocument11 pagesTopic 1: Introduction To Geria Nursing: Activity 1.1: Grandparents' LoveMarissa AsimNo ratings yet
- Propranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsDocument8 pagesPropranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsArlyn MarcelinoNo ratings yet
- Nutrition Education for an Underweight InfantDocument2 pagesNutrition Education for an Underweight InfantYzobel Phoebe ParoanNo ratings yet
- DP Discharge Plan@@@@@@@@Document6 pagesDP Discharge Plan@@@@@@@@Maemae SumalinogNo ratings yet
- Drug StudyDocument2 pagesDrug Studymegreen GamingNo ratings yet
- "Nisi Dominus Frustra" College of Nursing & Allied Health Sciences Maasin City, Southern LeyteDocument4 pages"Nisi Dominus Frustra" College of Nursing & Allied Health Sciences Maasin City, Southern Leytecoosa liquorsNo ratings yet
- NursesDocument36 pagesNursesGilbert BagsicNo ratings yet
- Physician's Orders for Admission and Treatment of Epigastric PainDocument4 pagesPhysician's Orders for Admission and Treatment of Epigastric PainJerremy LuqueNo ratings yet
- Summaries of El FiliDocument7 pagesSummaries of El FiliSanguinityNo ratings yet
- Steven Johnsons SyndromeDocument22 pagesSteven Johnsons SyndromeRoselene Mae MarasiganNo ratings yet
- Eating Disorder Manuscript ReportDocument16 pagesEating Disorder Manuscript ReportKeemuel LagriaNo ratings yet
- Eating DisordersDocument6 pagesEating DisordersKarthik SathyanNo ratings yet
- Dialysis Power PointDocument20 pagesDialysis Power PointJor GarciaNo ratings yet
- Reimbursement Claim FormDocument3 pagesReimbursement Claim FormGanesh Kumar100% (1)
- Epidemiology & Social Costs of Haemophilia in India: Review ArticleDocument13 pagesEpidemiology & Social Costs of Haemophilia in India: Review ArticleDharmendra B MistryNo ratings yet
- T Bar Clasp Retained Removable Partial Denture As An Alternative To Implant Based Prosthetic TreatmentDocument6 pagesT Bar Clasp Retained Removable Partial Denture As An Alternative To Implant Based Prosthetic TreatmentCurcubet OlgaNo ratings yet
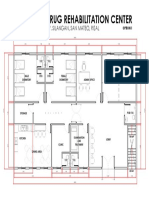
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNo ratings yet
- CEA DapagliflozinDocument11 pagesCEA DapagliflozinAe Navarut KongsalaNo ratings yet
- Reality TherapyDocument2 pagesReality TherapyAGLDNo ratings yet
- Nursing Process and Clinical Reasoning Cycle GuideDocument8 pagesNursing Process and Clinical Reasoning Cycle GuideTijanne-Jayde CunialNo ratings yet
- Collaborative TherapyDocument9 pagesCollaborative Therapyisiplaya2013No ratings yet
- MODULE 4. The Existential and Humanistic Approach To Counseling PsychotherapyDocument23 pagesMODULE 4. The Existential and Humanistic Approach To Counseling PsychotherapyCarmy Faith BaclayoNo ratings yet
- Revised Kanda NCPDocument3 pagesRevised Kanda NCPhaxa yzaNo ratings yet
- EBSCO Metadata 2023 04 19Document68 pagesEBSCO Metadata 2023 04 19psychologistnsmNo ratings yet
- Parkland Formula For Burns Calculated DecisionsDocument2 pagesParkland Formula For Burns Calculated DecisionsJulia Ines ObregonNo ratings yet
- Operating Room Surgical ProceduresDocument197 pagesOperating Room Surgical ProceduresChin Chan100% (6)
- DPT Doctor of Physiotherapy Program at Abu Zafar InstituteDocument44 pagesDPT Doctor of Physiotherapy Program at Abu Zafar InstituteAbdul basit KaleemNo ratings yet
- Colorectal CancerDocument23 pagesColorectal Cancerralph_gail100% (1)
- Introduction To HospitalsDocument15 pagesIntroduction To Hospitalskapgarg50% (2)
- Sigmund Freud's TheoryDocument22 pagesSigmund Freud's TheoryGil Mark B TOmas100% (2)
- Sensory Deprivation and Loss-4Document32 pagesSensory Deprivation and Loss-4Scott Daniel Phillips100% (1)
- New Grad Nurse Career SuccesDocument20 pagesNew Grad Nurse Career SuccesRacma Nawal100% (5)
- The Contribution of Carl Rogers and Humanistic Theory To The Understanding of Personality DevelopmentDocument13 pagesThe Contribution of Carl Rogers and Humanistic Theory To The Understanding of Personality DevelopmentOtto_CondliffeNo ratings yet
- Pathophysiology and Management of Psoriasis Diseas1Document28 pagesPathophysiology and Management of Psoriasis Diseas1Priyanka YadavNo ratings yet
- Assignment 3 4 Relapse Prevention Paper Brian MannDocument8 pagesAssignment 3 4 Relapse Prevention Paper Brian Mannapi-301673059No ratings yet
- Kuliah Dislipidemia UpdateDocument44 pagesKuliah Dislipidemia UpdateYudy Hardiyansah100% (1)
- Galler Spacing Technique (GST) ManualDocument44 pagesGaller Spacing Technique (GST) ManualDavid Galler100% (1)
- Job Shadowing PresentationDocument8 pagesJob Shadowing Presentationapi-360560383No ratings yet
- Diuretic DrugsDocument16 pagesDiuretic DrugslabillabooNo ratings yet
- Implant OcclusionDocument52 pagesImplant OcclusionElango25489100% (3)