You might also like
- Introduction to Cardiac UltrasoundDocument26 pagesIntroduction to Cardiac UltrasoundSandra GutierrezNo ratings yet
- Non-Invasive Cardiac ImagingDocument9 pagesNon-Invasive Cardiac Imagingoddone_outNo ratings yet
- Unit 1 Basics of Echocardiography and Cardiac DopplerDocument29 pagesUnit 1 Basics of Echocardiography and Cardiac DopplerJack TomarNo ratings yet
- Echocardiography General Principles and ExamplesDocument135 pagesEchocardiography General Principles and Examplesroseneels9No ratings yet
- Echo KibuddeDocument54 pagesEcho KibuddeTrevor Ishmael SiakambaNo ratings yet
- Echocardiography - LV FunctionDocument35 pagesEchocardiography - LV Functionusfcards100% (4)
- Systolic Function 2Document6 pagesSystolic Function 2FlorenceLorenzoNo ratings yet
- Adult Echocardiography Protocol 14 2Document10 pagesAdult Echocardiography Protocol 14 2api-349402240No ratings yet
- Coursebook-Echocardiography ch33Document21 pagesCoursebook-Echocardiography ch33ghina athirah100% (1)
- Study of Pediatric Congenital Cardiac Malformations by EchocardiographyDocument23 pagesStudy of Pediatric Congenital Cardiac Malformations by EchocardiographyRana Abd AlmugeethNo ratings yet
- 04 - Elements of EchocardiographyDocument56 pages04 - Elements of EchocardiographyMariana CabralNo ratings yet
- Basic EchocardiographyDocument63 pagesBasic EchocardiographyStella CooKeyNo ratings yet
- Introduction, Physics and KnobologyDocument47 pagesIntroduction, Physics and KnobologyMihaela LoghinNo ratings yet
- Ultrasound EchocardiographyDocument3 pagesUltrasound EchocardiographyDr. MLKNo ratings yet
- Holter Analysis Software FeaturesDocument27 pagesHolter Analysis Software FeaturesSuciu FlorinNo ratings yet
- Strain ImagingDocument54 pagesStrain ImagingKhalid Mehdi100% (1)
- Introduction to EchocardiographyDocument21 pagesIntroduction to EchocardiographyMaria EdelNo ratings yet
- Heart-Healthy Eating Asian Indian Style PDFDocument1 pageHeart-Healthy Eating Asian Indian Style PDFAnita Selvarajan ThangamNo ratings yet
- ASE HCM Poster FINALDocument2 pagesASE HCM Poster FINALBandar Alamri100% (1)
- Guidelines For Chamber QuantificationDocument1 pageGuidelines For Chamber QuantificationZoltán Tirczka100% (1)
- RV (Dys)function assessment by echocardiographyDocument52 pagesRV (Dys)function assessment by echocardiographyNag Mallesh RaoNo ratings yet
- Adult Congenital Heart Disease Board ReviewDocument79 pagesAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnNo ratings yet
- What Is EchocardiographyDocument18 pagesWhat Is EchocardiographyGeepi78No ratings yet
- Mechanical and Biological Valves - Key DifferencesDocument9 pagesMechanical and Biological Valves - Key DifferencesNavojit Chowdhury100% (1)
- Classic M Mode Echocardiography ECHOCARDIOGRAPHY BOARD REVIEWDocument73 pagesClassic M Mode Echocardiography ECHOCARDIOGRAPHY BOARD REVIEWMande SamuelNo ratings yet
- Echo CardiogramDocument2 pagesEcho CardiogramReyschelle Dela Rosa HernandezNo ratings yet
- Basic Echocardiography, MantapDocument54 pagesBasic Echocardiography, MantapDr Edi Hidayat50% (2)
- Echocardiography Function Guiline Image 추가Document105 pagesEchocardiography Function Guiline Image 추가stoicea catalin100% (1)
- Echocardiography: A Case-Based Review Case 2 Syncope Diastolic DysfunctionDocument34 pagesEchocardiography: A Case-Based Review Case 2 Syncope Diastolic DysfunctionDanielMinoPinoNo ratings yet
- Adult Echocardiography Protocol 13Document9 pagesAdult Echocardiography Protocol 13api-250194755100% (1)
- Prosth ValvesDocument74 pagesProsth ValvesRavi ZoreNo ratings yet
- Global Longitudinal StrainDocument7 pagesGlobal Longitudinal StrainBinod KumarNo ratings yet
- Luigi P. Badano, Roberto M. Lang, Denisa Muraru - Textbook of Three-Dimensional Echocardiography (2019, Springer International Publishing)Document367 pagesLuigi P. Badano, Roberto M. Lang, Denisa Muraru - Textbook of Three-Dimensional Echocardiography (2019, Springer International Publishing)Nicoletta Orphanou100% (1)
- Step by Step Echocardiography in Congenital Heart DiseasesDocument224 pagesStep by Step Echocardiography in Congenital Heart DiseasesEbookStore.DocNo ratings yet
- EKG in IHDDocument349 pagesEKG in IHDDinhLinh100% (1)
- Stress Echocardiography For Valvular Heart DiseaseDocument39 pagesStress Echocardiography For Valvular Heart DiseaseSofia KusumadewiNo ratings yet
- A Handbook On Clinical Echo CardiographyDocument71 pagesA Handbook On Clinical Echo Cardiographysri RamalakshmiNo ratings yet
- Anatomy of The Mitral Valve Understanding The Mitral Valve Complex in Mitral RegurgitationDocument7 pagesAnatomy of The Mitral Valve Understanding The Mitral Valve Complex in Mitral RegurgitationecocardioNo ratings yet
- @ebookmedicin Cardiology Clinics February 2017Document19 pages@ebookmedicin Cardiology Clinics February 2017mulyadiNo ratings yet
- Diagnosis and Management of The Neonate With Critical Congenital Heart DiseaseDocument35 pagesDiagnosis and Management of The Neonate With Critical Congenital Heart Diseasemotzco0% (1)
- Stress Echocardiography in Non-Ischaemic Heart DiseaseDocument39 pagesStress Echocardiography in Non-Ischaemic Heart DiseaseSohil3No ratings yet
- ECHO MASTERCLASS: A GUIDE TO ACCURATELY ASSESSING HEART VALVE DISEASEDocument136 pagesECHO MASTERCLASS: A GUIDE TO ACCURATELY ASSESSING HEART VALVE DISEASEVladlena Cucoș-CaraimanNo ratings yet
- CARDIAC CYCLE New For StudentDocument54 pagesCARDIAC CYCLE New For StudentDavi DzikirianNo ratings yet
- Dr. Alurkur's Book On Cardiology - 2Document85 pagesDr. Alurkur's Book On Cardiology - 2Bhattarai ShrinkhalaNo ratings yet
- Approach To A Patient With Congenital Heart DiseaseDocument164 pagesApproach To A Patient With Congenital Heart DiseaseCloudySkyNo ratings yet
- Quantification of Severity of Mitral Regurgitation With The New ASE GuidelinesDocument20 pagesQuantification of Severity of Mitral Regurgitation With The New ASE GuidelinesPanfilAlinaNo ratings yet
- CardiologyDocument149 pagesCardiologyMuhammad SyafiqNo ratings yet
- Guidelines TAVI TAVRDocument15 pagesGuidelines TAVI TAVRRossellaDisalvo100% (1)
- Aortic Root & Ascending Aortic Aneurysm Surgery OptionsTITLEDocument82 pagesAortic Root & Ascending Aortic Aneurysm Surgery OptionsTITLEMustafa KamalNo ratings yet
- Atrial Septial DefectDocument22 pagesAtrial Septial DefectJulie MckinneyNo ratings yet
- Mitral RegurgitationDocument10 pagesMitral RegurgitationWalter Saavedra YarlequeNo ratings yet
- Echocardiography Board Review: 400 Multiple Choice Questions With DiscussionFrom EverandEchocardiography Board Review: 400 Multiple Choice Questions With DiscussionNo ratings yet
- Pediatric Cardiology LectureDocument87 pagesPediatric Cardiology LectureMena HashemNo ratings yet
- Cardiology 2023 FinalDocument208 pagesCardiology 2023 FinalBelinda ELISHA100% (1)
- Natalya Master CardioDocument71 pagesNatalya Master CardioTaman Hoang100% (1)
- Principlesofdopplerultrasound 130514165605 Phpapp02Document92 pagesPrinciplesofdopplerultrasound 130514165605 Phpapp02csngiu100% (2)
- Saudi Commission Manual Classifies Health PractitionersDocument38 pagesSaudi Commission Manual Classifies Health Practitionerstoplexil100% (1)
- Strategic PlanDocument84 pagesStrategic PlanAurutchat VichaiditNo ratings yet
- Hemorragic Post PartumDocument10 pagesHemorragic Post PartumJihan NurlailaNo ratings yet
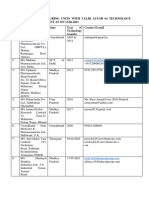
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Document5 pagesList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesNo ratings yet
- Chapter 8 ErgonomicsDocument18 pagesChapter 8 ErgonomicsAsif Rahman RaktimNo ratings yet
- Earnose 1 10091Document4 pagesEarnose 1 10091Annisa KartikasariNo ratings yet
- Pharmacokinetics and Pharmacodynamics of DrugsDocument11 pagesPharmacokinetics and Pharmacodynamics of Drugsahmalh01No ratings yet
- Laughter Discussion TopicDocument3 pagesLaughter Discussion Topicjelenap221219950% (1)
- Konsep Latihan Plyometric PDFDocument27 pagesKonsep Latihan Plyometric PDFDwinda Abi PermanaNo ratings yet
- Kerala PDocument106 pagesKerala PJeshiNo ratings yet
- PDF Created With Pdffactory Pro Trial Version: Page 1 of 3Document3 pagesPDF Created With Pdffactory Pro Trial Version: Page 1 of 3HindNo ratings yet
- Implants Session I Revised 21 Sept 2012Document17 pagesImplants Session I Revised 21 Sept 2012Norman AjxNo ratings yet
- Owbn Infernalism: Guide To Dark Thaumaturgy: A Sourcebook For One World by NightDocument35 pagesOwbn Infernalism: Guide To Dark Thaumaturgy: A Sourcebook For One World by NightJuhász ZoltánNo ratings yet
- Alabama Board of Medical Examiners Statement On Federal Pill Mill TakedownDocument103 pagesAlabama Board of Medical Examiners Statement On Federal Pill Mill TakedownAshley RemkusNo ratings yet
- Obesity Exercise PrescriptionDocument34 pagesObesity Exercise Prescriptionkhushbu88% (8)
- Philips Respironics Bipap ST Niv Noninvasive VentilatorDocument2 pagesPhilips Respironics Bipap ST Niv Noninvasive Ventilatorsonia87No ratings yet
- DR Wong Teck WeeipadDocument2 pagesDR Wong Teck Weeipadtwwong68No ratings yet
- Speech in ActionDocument160 pagesSpeech in ActionSplashXNo ratings yet
- List of Doctors by SpecialtyDocument6 pagesList of Doctors by Specialtykaushal shahNo ratings yet
- Nursing Comps Study GuideDocument15 pagesNursing Comps Study GuideforminskoNo ratings yet
- Return Demonstration: Urinary Catheterization Perineal CareDocument3 pagesReturn Demonstration: Urinary Catheterization Perineal CareDebbie beeNo ratings yet
- Yvonne Farrell Psycho Emotional NotesDocument10 pagesYvonne Farrell Psycho Emotional Notesபாலஹரிப்ரீதா முத்து100% (2)
- Cardiovascular Physiology Case 9Document50 pagesCardiovascular Physiology Case 9Kim AcostaNo ratings yet
- Blood Pressure Log 30Document2 pagesBlood Pressure Log 30Yousab KaldasNo ratings yet
- Older Adults Group PlanDocument31 pagesOlder Adults Group Planapi-316614503No ratings yet
- Spring 2011 21st AnniversaryDocument56 pagesSpring 2011 21st AnniversaryRajesh SekhriNo ratings yet
- Diagnostic Imaging Equipment & Consumables Laser PrintersDocument5 pagesDiagnostic Imaging Equipment & Consumables Laser Printersnanu_gomezNo ratings yet
- A Review On Acacia Arabica - An Indian Medicinal Plant: IJPSR (2012), Vol. 3, Issue 07 (Review Article)Document11 pagesA Review On Acacia Arabica - An Indian Medicinal Plant: IJPSR (2012), Vol. 3, Issue 07 (Review Article)amit chavanNo ratings yet
- Diatermo MB 122 and MB 160 Mono-Bipolar: Cautery & ElectrosurgeryDocument13 pagesDiatermo MB 122 and MB 160 Mono-Bipolar: Cautery & ElectrosurgeryDani Daniela100% (1)
- Complex Regional Pain Syndrome in Adults - Second Edition - 0 PDFDocument97 pagesComplex Regional Pain Syndrome in Adults - Second Edition - 0 PDFLotteDomineNo ratings yet