You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DetectionDocument8 pagesDetectionJanani GopalakrishnanNo ratings yet
- Comprehensive Format of Informed Consent in Research and Practice A Tool To Uphold The Ethical and Moral StandardsDocument9 pagesComprehensive Format of Informed Consent in Research and Practice A Tool To Uphold The Ethical and Moral StandardsJanani GopalakrishnanNo ratings yet
- Bleeding Disorders: Presented by Janani RGDocument43 pagesBleeding Disorders: Presented by Janani RGJanani GopalakrishnanNo ratings yet
- PH Modulation and Salivary Sugar Clearance of Different Chocolates in Children: A Randomized Clinical TrialDocument7 pagesPH Modulation and Salivary Sugar Clearance of Different Chocolates in Children: A Randomized Clinical TrialJanani GopalakrishnanNo ratings yet
- 4 160128142531Document150 pages4 160128142531Janani GopalakrishnanNo ratings yet
- Analgesics & Antibiotics in Pediatric DentistryDocument77 pagesAnalgesics & Antibiotics in Pediatric DentistryJanani Gopalakrishnan100% (3)
- DeskView Client 6 45 enDocument166 pagesDeskView Client 6 45 enRazvan22081997No ratings yet
- Hydrogen Production From Water Electrolysis: Role of CatalystsDocument23 pagesHydrogen Production From Water Electrolysis: Role of CatalystsFreddy Negron HuamaniNo ratings yet
- Research Proposal TransformerDocument3 pagesResearch Proposal Transformersohalder1026No ratings yet
- Programming in C - CPU Scheduling - Round RobinDocument3 pagesProgramming in C - CPU Scheduling - Round RobinGenus SumNo ratings yet
- Lab Guide #2 Coulombs LawDocument3 pagesLab Guide #2 Coulombs LawJoriel CruzNo ratings yet
- Hydraulic Calculation Forms and Water Supply Information: San José Fire DepartmentDocument3 pagesHydraulic Calculation Forms and Water Supply Information: San José Fire Departmentperie anugrahaNo ratings yet
- Flexible Perovskite Solar CellsDocument31 pagesFlexible Perovskite Solar CellsPEDRO MIGUEL SOLORZANO PICONNo ratings yet
- Chapter 3.1 - Igneous RockDocument64 pagesChapter 3.1 - Igneous Rockalvinllp83No ratings yet
- EMDCSS DatasheetDocument5 pagesEMDCSS DatasheetHoracio UlloaNo ratings yet
- Guar Gum: Product Data Sheet (PDS)Document1 pageGuar Gum: Product Data Sheet (PDS)Moatz HamedNo ratings yet
- TP 3017D Taman Angkasa Nuri - V01Document25 pagesTP 3017D Taman Angkasa Nuri - V01Najwa AzmanNo ratings yet
- 10 - Chapter 4 PDFDocument143 pages10 - Chapter 4 PDFKalyan ChakravarthyNo ratings yet
- Cronje Chemical 2010 PDFDocument569 pagesCronje Chemical 2010 PDFPara MoreNo ratings yet
- Intro To PVTDocument19 pagesIntro To PVTFernando OlaveoNo ratings yet
- Tetzaveh Parsha GematriaDocument1 pageTetzaveh Parsha GematriaRabbi Benyomin HoffmanNo ratings yet
- CP IMarEst Mitigation of Corrosion by Cathodic ProtectionDocument25 pagesCP IMarEst Mitigation of Corrosion by Cathodic Protectionjose yoyNo ratings yet
- Esam AliDocument23 pagesEsam AliYoussef AliNo ratings yet
- Analytical Investigation of Entropy Production With Convective Heat Transfer in Pressure Driven Flow of A Generalised Newtonian FluidDocument30 pagesAnalytical Investigation of Entropy Production With Convective Heat Transfer in Pressure Driven Flow of A Generalised Newtonian FluidUğur DemirNo ratings yet
- Optimum Policy ControlDocument4 pagesOptimum Policy ControlKimberly VargasNo ratings yet
- Woodward LeoPC Engineering ManualDocument40 pagesWoodward LeoPC Engineering ManualZafar AwanNo ratings yet
- Chemical Principles Notes Chapter 7Document86 pagesChemical Principles Notes Chapter 7Robert GardnerNo ratings yet
- Arthashastra: Citation NeededDocument4 pagesArthashastra: Citation NeededtusharNo ratings yet
- Maquinaria Forestal..Document14 pagesMaquinaria Forestal..Juan G ContrerasNo ratings yet
- Prob AnswersDocument4 pagesProb AnswersDaniel KirovNo ratings yet
- 16 Astral - Pool Heating 2008Document38 pages16 Astral - Pool Heating 2008drožmanićNo ratings yet
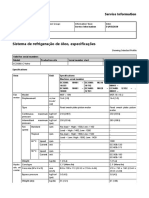
- Sistema de Refrigeração de Óleo, EspecificaçõesDocument2 pagesSistema de Refrigeração de Óleo, EspecificaçõesAlexandreNo ratings yet
- Test 4: GRE Real 19Document6 pagesTest 4: GRE Real 19rdrprsdm2640No ratings yet
- Upflow Anaerobic Sludge Blanket-Hollow Centered Packed Bed (UASB-HCPB) Reactor For Thermophilic Palm Oil Mill Effluent (POME) TreatmentDocument12 pagesUpflow Anaerobic Sludge Blanket-Hollow Centered Packed Bed (UASB-HCPB) Reactor For Thermophilic Palm Oil Mill Effluent (POME) TreatmentAgung Ariefat LubisNo ratings yet
- List of IEC StandardsDocument12 pagesList of IEC Standardsaravindeee08100% (1)
- Mobile HardwereDocument19 pagesMobile Hardwereanil8481No ratings yet