You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Which Activities Are The Circulating NurseDocument12 pagesWhich Activities Are The Circulating NurseDENNIS N. MUÑOZNo ratings yet
- Group 3 - Pharm 3DDocument3 pagesGroup 3 - Pharm 3DAila Marie ArandillaNo ratings yet
- CopdDocument89 pagesCopdVijayalaxmi KathareNo ratings yet
- Prometric 5 PDFDocument14 pagesPrometric 5 PDFFrancis Joseph Derla100% (2)
- 1 (7) Physiotherapy in Asthma Using The New Lotorp Method-IVA FAKHRIANI AMIRUDDINDocument4 pages1 (7) Physiotherapy in Asthma Using The New Lotorp Method-IVA FAKHRIANI AMIRUDDINIvha SmartNo ratings yet
- Leaflet Bricanyl TurbohalerDocument7 pagesLeaflet Bricanyl TurbohalerKrisna SyammaNo ratings yet
- Mexican Asthma Guidelines GUIMA 2017Document131 pagesMexican Asthma Guidelines GUIMA 2017Merk100% (1)
- AsthmaDocument4 pagesAsthmaIsabel CastilloNo ratings yet
- Gambaran Faal Paru Pada Pasien Asma Yang Melakukan Senam Asma Dengan Yang Tidak Melakukan Senam Asma Uci Tama Azilla Sri Melati Munir Eka BebasariDocument17 pagesGambaran Faal Paru Pada Pasien Asma Yang Melakukan Senam Asma Dengan Yang Tidak Melakukan Senam Asma Uci Tama Azilla Sri Melati Munir Eka BebasariiqbalNo ratings yet
- Pre Test and Post TestDocument27 pagesPre Test and Post TestMATALANG GRACENo ratings yet
- Bronchial Asthma Case StudyDocument52 pagesBronchial Asthma Case StudyYang ChimsNo ratings yet
- Páginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-1Document1 pagePáginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-1Sotfonic SotfonicNo ratings yet
- Respiratory System AssignmentDocument3 pagesRespiratory System AssignmentzainaNo ratings yet
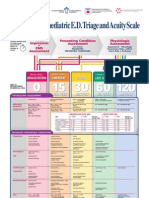
- Paediatric Triage PosterDocument1 pagePaediatric Triage PosterGenaro Olmos Garcia100% (2)
- Peak Expiratory FlowDocument1 pagePeak Expiratory FlowMizna JanihimNo ratings yet
- Pulmonology Review: Key Topics in Lung Disease ManagementDocument23 pagesPulmonology Review: Key Topics in Lung Disease ManagementAsif Newaz100% (1)
- School Based Vaccination For Import To QVACDocument3 pagesSchool Based Vaccination For Import To QVACMarita SibugNo ratings yet
- Sulfur Trioxide and OleumDocument21 pagesSulfur Trioxide and OleumEduardo Magallon100% (1)
- Asthma COPD CounsellingDocument3 pagesAsthma COPD CounsellingAnonymous 9dVZCnTXSNo ratings yet
- Argumentative EssayDocument9 pagesArgumentative Essayapi-412321892No ratings yet
- Lagundi Leaves Research PaperDocument6 pagesLagundi Leaves Research Paperfvg1rph4100% (1)
- bIOLOGIC cRISIS FINAL QUIZ pHARMACOCHENETICSDocument35 pagesbIOLOGIC cRISIS FINAL QUIZ pHARMACOCHENETICSSusan MaglaquiNo ratings yet
- Clinical Pharmacology of Bronchodilator MedicationsDocument22 pagesClinical Pharmacology of Bronchodilator MedicationsGal ChrisNo ratings yet
- Clin Med I Exam 1 - CS Study GuideDocument17 pagesClin Med I Exam 1 - CS Study GuidecrystalsheNo ratings yet
- Test Bank For Human Diseases 3rd Edition NeighborsDocument24 pagesTest Bank For Human Diseases 3rd Edition NeighborsBarbaraHernandezimgf100% (44)
- Ealing Paces 2014Document100 pagesEaling Paces 2014Cindy WongNo ratings yet
- BIOC3364 - 2021 Lecture Notes AsthmaDocument26 pagesBIOC3364 - 2021 Lecture Notes AsthmachrystalNo ratings yet
- Dr. Rishi Pal: Asstt. ProfessorDocument40 pagesDr. Rishi Pal: Asstt. ProfessortamaNo ratings yet
- Assess Ability To Learn or Perform Desired Health-Related CareDocument6 pagesAssess Ability To Learn or Perform Desired Health-Related CareMarielle J GarciaNo ratings yet
- Forced Expiration Exercises in Asthma and Their Effect On FEVDocument3 pagesForced Expiration Exercises in Asthma and Their Effect On FEVdelphineNo ratings yet