You might also like
- Magical Industrial RevolutionDocument156 pagesMagical Industrial RevolutionUgly Panda100% (12)
- Vitamin D3Document29 pagesVitamin D3Ambreen AmirNo ratings yet
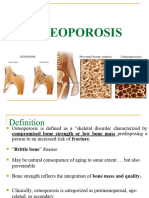
- Osteoporosis: Prepared By: Md. Giash Uddin Lecturer, Dept. of Pharmacy University of ChittagongDocument30 pagesOsteoporosis: Prepared By: Md. Giash Uddin Lecturer, Dept. of Pharmacy University of Chittagongsamiul bashirNo ratings yet
- Pinochle Rules GuideDocument2 pagesPinochle Rules GuidepatrickNo ratings yet
- ThiruppavaiDocument157 pagesThiruppavaiajiva_rts100% (49)
- Understanding Death Through the Life SpanDocument52 pagesUnderstanding Death Through the Life SpanKaren HernandezNo ratings yet
- Phonetics Exercises PDFDocument2 pagesPhonetics Exercises PDFShanti YuliastitiNo ratings yet
- Mayo Clinic Guide to Preventing & Treating Osteoporosis: Keeping Your Bones Healthy and Strong to Reduce Your Risk of FractureFrom EverandMayo Clinic Guide to Preventing & Treating Osteoporosis: Keeping Your Bones Healthy and Strong to Reduce Your Risk of FractureRating: 2 out of 5 stars2/5 (1)
- OsteoporosisDocument43 pagesOsteoporosisMuna Hassan Mustafa100% (1)
- Everything You Need to Know About OsteoporosisDocument33 pagesEverything You Need to Know About OsteoporosisCiptadi Permana Wijaya100% (1)
- OsteoporosisDocument9 pagesOsteoporosisRenuka Sivaram71% (7)
- Running Head: OSTEOPOROSIS 1Document7 pagesRunning Head: OSTEOPOROSIS 1AssignmentLab.comNo ratings yet
- Osteoporosis: Hani Abu DiehDocument24 pagesOsteoporosis: Hani Abu DiehAngelic khan100% (1)
- Pratt & Whitney Engine Training ResourcesDocument5 pagesPratt & Whitney Engine Training ResourcesJulio Abanto50% (2)
- 6199026M2 Pre Powershift and Synchro Shuttle TX750 TX760 TX860Document394 pages6199026M2 Pre Powershift and Synchro Shuttle TX750 TX760 TX860Gustavo100% (7)
- Isavasya UpanishadDocument5 pagesIsavasya UpanishadskmrrlNo ratings yet
- 2023 Civil LawDocument7 pages2023 Civil LawJude OnrubiaNo ratings yet
- Metabolic Bone Disorders: Osteoporosis and ManagementDocument35 pagesMetabolic Bone Disorders: Osteoporosis and Managementkelemwork WaleNo ratings yet
- Novartis Osteoporosis Slide KitDocument42 pagesNovartis Osteoporosis Slide KitShravanti SatyanandNo ratings yet
- OsteoporosisDocument22 pagesOsteoporosisPrachi DSaNo ratings yet
- Osteoporosis: Blondina Marpaung Rheumatology Division Internal Department Medical Faculty USU - MedanDocument47 pagesOsteoporosis: Blondina Marpaung Rheumatology Division Internal Department Medical Faculty USU - MedanFadhly SharimanNo ratings yet
- Osteoporosis: Dr. Lubna DwerijDocument26 pagesOsteoporosis: Dr. Lubna DwerijNoor MajaliNo ratings yet
- Osteoporosis: The Silent Bone DiseaseDocument15 pagesOsteoporosis: The Silent Bone Diseaseعبدالرحمن علىNo ratings yet
- Osteoporosis: Screening, Prevention, and ManagementDocument20 pagesOsteoporosis: Screening, Prevention, and ManagementBernardo RomeroNo ratings yet
- OsteoporosisDocument51 pagesOsteoporosissarguss14No ratings yet
- Skeletal System Diseases and DisordersDocument32 pagesSkeletal System Diseases and DisordersPatrisha Georgia AmitenNo ratings yet
- Dissertation OsteoporosisDocument5 pagesDissertation OsteoporosisWriteMyPaperFastCanada100% (1)
- SOGOsteoporosisforPublic 1Document37 pagesSOGOsteoporosisforPublic 1Muhammad AdnanNo ratings yet
- 7 Ways To Save Your Bones: Health / Body / Life / SoulDocument4 pages7 Ways To Save Your Bones: Health / Body / Life / SoulGregorio PetteNo ratings yet
- Supplement Guide Bone HealthDocument37 pagesSupplement Guide Bone HealthJeff BanksNo ratings yet
- Diseases of The Skeletal SystemDocument16 pagesDiseases of The Skeletal SystemNoor-E-Khadiza ShamaNo ratings yet
- Understanding OsteoporosisDocument28 pagesUnderstanding OsteoporosisDewy Shinta PagalaNo ratings yet
- Bone Markers Univ West APC Feb 2013Document82 pagesBone Markers Univ West APC Feb 2013monday125No ratings yet
- Osteoporosis Thesis PDFDocument6 pagesOsteoporosis Thesis PDFmonicabogdaneverett100% (2)
- Cooper C, Campion G, Melton LJ, 3rd. Hip Fractures in The Elderly: A World-Wide Projection. Osteoporosis Int. 1992 2 (6) :285-289Document5 pagesCooper C, Campion G, Melton LJ, 3rd. Hip Fractures in The Elderly: A World-Wide Projection. Osteoporosis Int. 1992 2 (6) :285-289Noor-E-Khadiza ShamaNo ratings yet
- Bone Health and Osteoporosis: A Guide For Asian Women Age 50 and OlderDocument4 pagesBone Health and Osteoporosis: A Guide For Asian Women Age 50 and OlderOlivia SuritnoNo ratings yet
- OsteoporosisDocument6 pagesOsteoporosiskingNo ratings yet
- OsteoporosisDocument6 pagesOsteoporosiskingNo ratings yet
- OsteoporosisDocument6 pagesOsteoporosiskingNo ratings yet
- OsteoporosisDocument6 pagesOsteoporosiskingNo ratings yet
- Chapter 23: Osteoporosis of The SpineDocument15 pagesChapter 23: Osteoporosis of The SpineTraian UrsuNo ratings yet
- OsteoporosisDocument13 pagesOsteoporosisRuaa MalekNo ratings yet
- Bone AbdallahDocument2 pagesBone Abdallahعبدالله بدرانNo ratings yet
- Osteoporosis For BonesDocument24 pagesOsteoporosis For BonesRoking KumarNo ratings yet
- OsteoporosisDocument35 pagesOsteoporosisFarida Abo ElmagdNo ratings yet
- OsteoporosisDocument12 pagesOsteoporosisAzharul Islam ArjuNo ratings yet
- OsteoporosisDocument57 pagesOsteoporosisViviViviNo ratings yet
- MT16 QSU60104 M221 | MUSCLE AND BONE PROBLEMSDocument6 pagesMT16 QSU60104 M221 | MUSCLE AND BONE PROBLEMSFOONG YI KUAN MoeNo ratings yet
- Osteoporosis: Signs and SymptomsDocument9 pagesOsteoporosis: Signs and SymptomschelseachoirNo ratings yet
- Osteoporosis 16Document12 pagesOsteoporosis 16Diego AramburoNo ratings yet
- OsteoporosisDocument19 pagesOsteoporosissaminashrafi003No ratings yet
- Anatomy Learning Journalunit2fDocument3 pagesAnatomy Learning Journalunit2fCharity NyirongoNo ratings yet
- Bone Abnormalities: Causes, Prevention and CareTITLEDocument2 pagesBone Abnormalities: Causes, Prevention and CareTITLEMary Pauline G. CamposNo ratings yet
- Herbal Treatment For Osteoporosis: A Current Review: Ping Chung Leung, Wing Sum SiuDocument6 pagesHerbal Treatment For Osteoporosis: A Current Review: Ping Chung Leung, Wing Sum Siusiska khairNo ratings yet
- Osteomalacia and Osteoporosis Causes, Symptoms, and TreatmentDocument28 pagesOsteomalacia and Osteoporosis Causes, Symptoms, and TreatmentReginette Pisalbo ChanNo ratings yet
- G24 Fragility FracturesDocument38 pagesG24 Fragility FracturesDeep Katyan DeepNo ratings yet
- OsteoporosisDocument93 pagesOsteoporosisprotikNo ratings yet
- Wilson, 2019 PDFDocument6 pagesWilson, 2019 PDFadi pranotoNo ratings yet
- Osteoporosis: Done By: Dalal Hussain AlanaziDocument15 pagesOsteoporosis: Done By: Dalal Hussain AlanazidallasNo ratings yet
- OsteoporosisDocument19 pagesOsteoporosisTsedhonNo ratings yet
- Osteoporosis and AsthakshayaDocument8 pagesOsteoporosis and AsthakshayaBala Kiran GaddamNo ratings yet
- OsteoporosisDocument16 pagesOsteoporosisDe Sesto Rhys CarloNo ratings yet
- Abh Basiccommunitytalk 2017 Final VersionDocument34 pagesAbh Basiccommunitytalk 2017 Final VersionAnggi D.WijayantiNo ratings yet
- Bio Project File 2Document19 pagesBio Project File 2jiya singhNo ratings yet
- Osteoporosis: Why It Affects More Women Than MenDocument5 pagesOsteoporosis: Why It Affects More Women Than MenKaye CortadoNo ratings yet
- Osteoporosis: Why It Affects More Women Than MenDocument5 pagesOsteoporosis: Why It Affects More Women Than MenKaye CortadoNo ratings yet
- Nutrition Research EssayDocument6 pagesNutrition Research Essayapi-301415536No ratings yet
- Role of Exercise in Post-Menopausal WomenDocument15 pagesRole of Exercise in Post-Menopausal Womenapi-304463583No ratings yet
- Pharmaceutical Generics Available As InfusionsDocument7 pagesPharmaceutical Generics Available As InfusionsAmbreen AmirNo ratings yet
- HypertensionDocument15 pagesHypertensionAmbreen AmirNo ratings yet
- HypertensionDocument15 pagesHypertensionAmbreen AmirNo ratings yet
- Safety & Use of CiprofloxacinDocument9 pagesSafety & Use of CiprofloxacinAmbreen AmirNo ratings yet
- B1 Grammar and VocabularyDocument224 pagesB1 Grammar and VocabularyTranhylapNo ratings yet
- Value Creation-How-Can-The-Semiconductor-Industry-Keep-Outperforming-FinalDocument7 pagesValue Creation-How-Can-The-Semiconductor-Industry-Keep-Outperforming-FinalJoão Vitor RibeiroNo ratings yet
- Budget Planner Floral Style-A5Document17 pagesBudget Planner Floral Style-A5Santi WidyaninggarNo ratings yet
- Work-Life Balance: Before ReadingDocument5 pagesWork-Life Balance: Before ReadingJulianna AvilaNo ratings yet
- CPB145 CVTDocument1 pageCPB145 CVTDantiancNo ratings yet
- Java Thread Priority in MultithreadingDocument3 pagesJava Thread Priority in MultithreadingMITALI SHARMANo ratings yet
- Planned Parenthood Great NorthWestDocument10 pagesPlanned Parenthood Great NorthWestKate AndersonNo ratings yet
- Council Of Architecture Scale Of ChargesDocument4 pagesCouncil Of Architecture Scale Of ChargesAshwin RajendranNo ratings yet
- Plants Promoting Happiness: The Effect of Indoor Plants on MoodDocument11 pagesPlants Promoting Happiness: The Effect of Indoor Plants on MoodWil UfanaNo ratings yet
- CARAGA REGIONAL SCIENCE HIGH SCHOOL ASSESSMENT #1Document3 pagesCARAGA REGIONAL SCIENCE HIGH SCHOOL ASSESSMENT #1Joana Jean SuymanNo ratings yet
- MICROHARDNESS TESTER HMV-2 - SeriesDocument9 pagesMICROHARDNESS TESTER HMV-2 - SeriesRicoNo ratings yet
- Tarea 1Document36 pagesTarea 1LUIS RVNo ratings yet
- Miles and Snow's Organizational StrategiesDocument15 pagesMiles and Snow's Organizational StrategiesVirat SahNo ratings yet
- Repeaters XE PDFDocument12 pagesRepeaters XE PDFenzzo molinariNo ratings yet
- UT Dallas Syllabus For Chem2323.001.10s Taught by Sergio Cortes (Scortes)Document9 pagesUT Dallas Syllabus For Chem2323.001.10s Taught by Sergio Cortes (Scortes)UT Dallas Provost's Technology GroupNo ratings yet
- Semester 3 SyllabusDocument12 pagesSemester 3 SyllabusFuggi JaanNo ratings yet
- Inmarsat M2M Terminal ComparisonDocument2 pagesInmarsat M2M Terminal Comparisonmaruka33No ratings yet
- EN4264 Final Essay - GeraldineDocument25 pagesEN4264 Final Essay - GeraldineGeraldine WongNo ratings yet
- Samonte Vs CADocument7 pagesSamonte Vs CAMaricel Caranto FriasNo ratings yet
- Yale Film Analysis WebsiteDocument5 pagesYale Film Analysis WebsiteizmcnortonNo ratings yet
- Failure CountersDocument28 pagesFailure CountersБотирали АзибаевNo ratings yet