You might also like
- Absorption of DrugsDocument41 pagesAbsorption of DrugsSibtain100% (2)
- Pharmacokinetics AbsorptionDocument27 pagesPharmacokinetics AbsorptionchondroboraNo ratings yet
- Pharma 1.2 - Pharmacokinetics (Wini Ong) PDFDocument11 pagesPharma 1.2 - Pharmacokinetics (Wini Ong) PDFVon Javier GamateroNo ratings yet
- Dosage Form Design: Pharmaceutical ConsiderationsDocument9 pagesDosage Form Design: Pharmaceutical ConsiderationsVIJAY KUMAR TIRUKKACHINo ratings yet
- 4-Pharmacokinetics IDocument88 pages4-Pharmacokinetics IMarc Imhotep Cray, M.D.No ratings yet
- PharmacologyDocument19 pagesPharmacologyBhanu K Prakash100% (1)
- Histamine and Antihistamines. NotesDocument5 pagesHistamine and Antihistamines. NotesSubha2000100% (1)
- Beta-lactam antibiotics cell wall synthesis inhibitorsDocument29 pagesBeta-lactam antibiotics cell wall synthesis inhibitorsRen PastelNo ratings yet
- Pharmacokinetics: Saminathan Kayarohanam M.Pharm, M.B.A, PHDDocument26 pagesPharmacokinetics: Saminathan Kayarohanam M.Pharm, M.B.A, PHDSaminathan KayarohanamNo ratings yet
- Nsaids, Dmards, Nonopioid Analgesics, Drugs Used in Gout: DR - Minerva P. Calimag, MD - September 6, 2019Document9 pagesNsaids, Dmards, Nonopioid Analgesics, Drugs Used in Gout: DR - Minerva P. Calimag, MD - September 6, 2019Eryll Paolo Alea100% (2)
- Pharmacokinetics & Pharmacodynamics ExplainedDocument2 pagesPharmacokinetics & Pharmacodynamics Explainedgeldevera100% (1)
- Factors Influencing GI Absorption of DrugDocument11 pagesFactors Influencing GI Absorption of DrugjeorajaNo ratings yet
- Introduction To PharmacologyDocument28 pagesIntroduction To Pharmacologynadar shahNo ratings yet
- Basic Concept On ToxicologyDocument40 pagesBasic Concept On Toxicologyadel santosNo ratings yet
- Gpat 2020 Achiver 2400 Mcqs Exp - CDocument376 pagesGpat 2020 Achiver 2400 Mcqs Exp - CRohit patelNo ratings yet
- Receptors and PharmacodynamicsDocument78 pagesReceptors and PharmacodynamicsMuhammad Bilal Bin Amir100% (1)
- Pharmacokinetic One Compartment ModelDocument28 pagesPharmacokinetic One Compartment ModelAmy Yuen100% (1)
- General Pharmacology (1-7)Document7 pagesGeneral Pharmacology (1-7)LotfyAdel100% (1)
- 29880020: Antiepileptic Drugs in Critically Ill PatientsDocument12 pages29880020: Antiepileptic Drugs in Critically Ill PatientsEward Rod SalNo ratings yet
- General Pharmacology-QuestionDocument4 pagesGeneral Pharmacology-Questionlina amjadNo ratings yet
- Drug Elimination KineticsDocument12 pagesDrug Elimination KineticsBenjel AndayaNo ratings yet
- Intro PK PD Genomics - PharmaDocument110 pagesIntro PK PD Genomics - PharmaKenneth NuñezNo ratings yet
- Drug DistributionDocument49 pagesDrug DistributionDrAmit VermaNo ratings yet
- Chapter 43 - Beta-LactamDocument7 pagesChapter 43 - Beta-LactamErika De JesusNo ratings yet
- Transes PharmacodynamicsDocument36 pagesTranses PharmacodynamicsGwyneth Koleen Lopez100% (1)
- Introduction of PharmacologyDocument33 pagesIntroduction of PharmacologykayarohanamNo ratings yet
- Pharmacology Practical Manual - Student Copy2Document11 pagesPharmacology Practical Manual - Student Copy2NareshNo ratings yet
- Introduction To PharmacogenomicsDocument35 pagesIntroduction To Pharmacogenomicssazaki224No ratings yet
- Clinical Toxicology Page 1 of 10: TH TH TH THDocument10 pagesClinical Toxicology Page 1 of 10: TH TH TH THKitkat Casacop100% (1)
- Pharma 1.2 - Pharmacokinetics (Vision) PDFDocument14 pagesPharma 1.2 - Pharmacokinetics (Vision) PDFVon Javier GamateroNo ratings yet
- Notes in PharmacologyDocument96 pagesNotes in Pharmacologydmd_2dd50% (2)
- Introduction To BiopharmaceuticsDocument106 pagesIntroduction To BiopharmaceuticsHely Patel100% (1)
- Autacoid PharmacologyDocument38 pagesAutacoid PharmacologyAakkkNo ratings yet
- Anticancer Drugs ClassificationDocument19 pagesAnticancer Drugs ClassificationMuhammad Raza100% (1)
- Antiplatelet and Thrombolytic DrugsDocument48 pagesAntiplatelet and Thrombolytic DrugsNofa PuspitaNo ratings yet
- Pharmacology ReviewDocument172 pagesPharmacology ReviewJan Patrick Arrieta100% (1)
- Biopharmaceutics: GSDMSFI - BS Pharmacy 3Document11 pagesBiopharmaceutics: GSDMSFI - BS Pharmacy 3Majeddah Aliudin TalambunganNo ratings yet
- Introduction to Microbiology: Understanding MicrobesDocument55 pagesIntroduction to Microbiology: Understanding MicrobesRenel Esteves RestauroNo ratings yet
- Final Answer of PharmacologyDocument45 pagesFinal Answer of Pharmacologynidhhu100% (1)
- Pharmacotherapeutics UNIT1Document44 pagesPharmacotherapeutics UNIT1Bharti ChauhanNo ratings yet
- BASIC PHARMACOKINETICS - CHAPTER 11: Multicompartment ModelDocument65 pagesBASIC PHARMACOKINETICS - CHAPTER 11: Multicompartment ModelDrHeba100% (1)
- Pharmacology OverviewDocument95 pagesPharmacology OverviewMiguel CuevasNo ratings yet
- Basic Principles of PharmacologyDocument75 pagesBasic Principles of PharmacologyJessica Febrina Wuisan100% (1)
- Pharmacology I MCQs on General Pharmacological PrinciplesDocument34 pagesPharmacology I MCQs on General Pharmacological PrinciplesAman Gurjar100% (1)
- RECEPTORSDocument22 pagesRECEPTORSpharmazone4u100% (1)
- Autocoids and Their AntagonistsDocument19 pagesAutocoids and Their AntagonistsHossein Sehati100% (1)
- MCQ PharmacologyDocument140 pagesMCQ PharmacologyVazeerNo ratings yet
- Cholinergic DrugsDocument44 pagesCholinergic Drugskhuzaima9100% (1)
- Cholinergic and AnticholinergicDocument77 pagesCholinergic and Anticholinergicsweta sumanNo ratings yet
- Vanishing and Cold Creams PPT - 3.9.20Document24 pagesVanishing and Cold Creams PPT - 3.9.20madhanraj7996No ratings yet
- BiopharmaceuticsDocument13 pagesBiopharmaceuticsAngeli Marie PadillaNo ratings yet
- Lead Identification and Lead Optimization: An Over View of Modern Drug Discovery ProcessDocument21 pagesLead Identification and Lead Optimization: An Over View of Modern Drug Discovery ProcessTia Rahayu AnggrainiNo ratings yet
- ملخص من علم الأدوية وعلم الصيدلانياتDocument101 pagesملخص من علم الأدوية وعلم الصيدلانياتAbdennour AyoubNo ratings yet
- Clinical PharmacologDocument81 pagesClinical PharmacologSHILOTANo ratings yet
- RINJUDocument35 pagesRINJUதீபன்குமார் கதிரேசன்100% (1)
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (2)
- Pharmacotherapeutics 140828123349 Phpapp02Document14 pagesPharmacotherapeutics 140828123349 Phpapp02Anonymous s9i0WyKF200% (1)
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- What Is Rheumatoid ArthritisDocument16 pagesWhat Is Rheumatoid ArthritisDurge Raj GhalanNo ratings yet
- SilicosisDocument11 pagesSilicosisDurge Raj GhalanNo ratings yet
- Pharmacology1Medical PharmacologyDocument9 pagesPharmacology1Medical PharmacologyNagrani PuttaNo ratings yet
- Phathophysiology2 (Water and Electrolytes Balance and Imbalance)Document61 pagesPhathophysiology2 (Water and Electrolytes Balance and Imbalance)Durge Raj Ghalan100% (2)
- Pharmacology2 (Drug Receptors & Pharmacodynamics)Document58 pagesPharmacology2 (Drug Receptors & Pharmacodynamics)Durge Raj Ghalan100% (2)
- Pathophysiology 1 (Conspectus of Disease)Document84 pagesPathophysiology 1 (Conspectus of Disease)Durge Raj Ghalan100% (1)
- Phathology-3 (Disorders of Blood Circulation)Document146 pagesPhathology-3 (Disorders of Blood Circulation)Durge Raj Ghalan100% (1)
- Mero Hunan YatraDocument5 pagesMero Hunan YatraDurge Raj GhalanNo ratings yet
- Pathology-1 (Introduction To Pathology)Document87 pagesPathology-1 (Introduction To Pathology)Durge Raj Ghalan67% (6)
- Pathology-2 (Cell Injury & Healing)Document95 pagesPathology-2 (Cell Injury & Healing)Durge Raj Ghalan100% (1)
- Australian Model Railway - February 2016Document80 pagesAustralian Model Railway - February 2016Meep100% (5)
- FA2-FA2 5 Service Manual Parts ListDocument61 pagesFA2-FA2 5 Service Manual Parts ListERNESTO NEGRETENo ratings yet
- 32 12 16 - Asphalt PavingDocument4 pages32 12 16 - Asphalt PavingSteve LezamaNo ratings yet
- Steel Casting HandboockDocument446 pagesSteel Casting Handboockomar quiñonesNo ratings yet
- Airbus A320 PDFDocument19 pagesAirbus A320 PDFntdkhanNo ratings yet
- 9 11 Commission ACARS Assessment PDFDocument57 pages9 11 Commission ACARS Assessment PDFAidan MonaghanNo ratings yet
- Route 534 Santa Monica MalibuDocument3 pagesRoute 534 Santa Monica MalibudazulzulNo ratings yet
- Af521 (2012) - ManDocument22 pagesAf521 (2012) - ManNUCLEONIX SYSTEMS PVT LTDNo ratings yet
- Proforma Invoice for Biotech Analyzer ExportDocument1 pageProforma Invoice for Biotech Analyzer ExportJosé Carlos López LuqueNo ratings yet
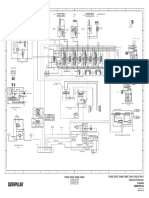
- TH336, TH337, TH406, TH407, TH414, TH514, TH417 Hydraulic Schematic TH336, TH337, TH406, TH407Document2 pagesTH336, TH337, TH406, TH407, TH414, TH514, TH417 Hydraulic Schematic TH336, TH337, TH406, TH407مهدي شقرونNo ratings yet
- Logistics Sheet All County ChorusDocument1 pageLogistics Sheet All County Chorusapi-367519610No ratings yet
- S/N Cat: Safa Defect Categorization AerospaceDocument36 pagesS/N Cat: Safa Defect Categorization AerospaceZain MaqsoodNo ratings yet
- 1 Medio Ruta de Aprendizaje 07 - 08 - 09Document32 pages1 Medio Ruta de Aprendizaje 07 - 08 - 09nanolakesNo ratings yet
- NISSAN KICKS SUV Earns 34 Safety PointsDocument4 pagesNISSAN KICKS SUV Earns 34 Safety PointsGalih PnNo ratings yet
- Cellular Transport Study Guide PDFDocument4 pagesCellular Transport Study Guide PDFJESUS EDUARDO CARBONO NIEBLESNo ratings yet
- B737 Load SheetDocument2 pagesB737 Load Sheetkanavkashyap85% (13)
- Kamana Sewa Bikash Bank Summer ReportDocument42 pagesKamana Sewa Bikash Bank Summer Reportumesh aryaNo ratings yet
- RLM 252 MODU 8 06 WDocument5 pagesRLM 252 MODU 8 06 WzaladsNo ratings yet
- AvayaDocument67 pagesAvayaEbrahim JasimNo ratings yet
- Siemens Etu45b ManualDocument24 pagesSiemens Etu45b ManualVictor Godoy0% (2)
- 1285Document11 pages1285Kaushik SenguptaNo ratings yet
- Equipment, Navigation and FacilitiesDocument9 pagesEquipment, Navigation and FacilitiesJuly TadeNo ratings yet
- MTOM and TL QuestionsDocument3 pagesMTOM and TL QuestionsHazel NightshadeNo ratings yet
- Intralogistics Automation in The Automotive IndustryDocument12 pagesIntralogistics Automation in The Automotive IndustrycyrilNo ratings yet
- A2 Shipboard Fittings and Supporting Hull Structures Associated With Towing and Mooring On Conventional Vessels A2Document6 pagesA2 Shipboard Fittings and Supporting Hull Structures Associated With Towing and Mooring On Conventional Vessels A2tonyNo ratings yet
- Internship Journal Week 1 FormattedDocument2 pagesInternship Journal Week 1 FormattedFarhan Israq AhmedNo ratings yet
- Automotive Design Course IndiaDocument17 pagesAutomotive Design Course Indiamq23No ratings yet
- Oil Type For BPDocument4 pagesOil Type For BPRisza AnugrahNo ratings yet
- Oarr 10000310 1 PDFDocument520 pagesOarr 10000310 1 PDFyoussefNo ratings yet
- MCC DSR Rate AnalysisDocument280 pagesMCC DSR Rate AnalysisAbhijeet VardheNo ratings yet