You might also like
- IKM Cohort StudyDocument88 pagesIKM Cohort Studyankirana02No ratings yet
- Case Control Study DesignDocument15 pagesCase Control Study Designgeorgeloto12No ratings yet
- Hang OutDocument92 pagesHang OutMadhu UpadhyayNo ratings yet
- Case Control StudyDocument6 pagesCase Control Studyphian0No ratings yet
- Cohort StudyDocument37 pagesCohort Studygilbert2691No ratings yet
- Epidemiologic Study Designs: Dr. Sunita Dodani Assistant Professor Family Medicine, CHSDocument23 pagesEpidemiologic Study Designs: Dr. Sunita Dodani Assistant Professor Family Medicine, CHSShubha DavalgiNo ratings yet
- Epidemiology 2Document54 pagesEpidemiology 2oheneapeahrita100% (2)
- Bisotat For MlsDocument57 pagesBisotat For MlsABAYNo ratings yet
- LEC 3 Study DesignsDocument44 pagesLEC 3 Study DesignsFaint Faint100% (1)
- Study Designs in Epidemiologic Research Chronic DiseasesDocument51 pagesStudy Designs in Epidemiologic Research Chronic DiseasesLeonel Nkweti100% (2)
- Epidemic Investigation 2Document10 pagesEpidemic Investigation 2Den Anacay100% (1)
- Study Design Contingency TablesDocument41 pagesStudy Design Contingency TablesDaniel Bondoroi100% (1)
- Epidemiological StudiesDocument21 pagesEpidemiological Studiespriyaa100% (1)
- Epidemiological Study DesignsDocument60 pagesEpidemiological Study DesignsAnn Hill100% (1)
- Animal Models in Experimental Gastric Ulcer Screening-A ReviewDocument6 pagesAnimal Models in Experimental Gastric Ulcer Screening-A Reviewnareshph28No ratings yet
- Epidemiology EpidemiologyDocument13 pagesEpidemiology EpidemiologyBiratNagarNo ratings yet
- Concept of DiseaseDocument80 pagesConcept of DiseaseMamata ManandharNo ratings yet
- Biostat Lecture NoteDocument116 pagesBiostat Lecture NoteMiki SileshiNo ratings yet
- Biostat Q2Document8 pagesBiostat Q2Ruba GhanimNo ratings yet
- EpidemiologyDocument40 pagesEpidemiologyCharityOchiengNo ratings yet
- Hierarchy of Epidemiologic Study Design: Tower & Spector, 2007Document42 pagesHierarchy of Epidemiologic Study Design: Tower & Spector, 2007Aslam BajwaNo ratings yet
- Epidemiology Principles and Methods Prof Bhisma MurtiDocument32 pagesEpidemiology Principles and Methods Prof Bhisma Murtievy_silviania8873100% (1)
- Study DesignDocument34 pagesStudy DesignVikashgtmNo ratings yet
- Analytical EpidemiologyDocument64 pagesAnalytical EpidemiologyQueency Dangilan100% (1)
- Introduction To BiostatisticsDocument64 pagesIntroduction To BiostatisticsFadel DeebNo ratings yet
- Study DesignDocument45 pagesStudy DesignDeepak SharmaNo ratings yet
- Basic BioostatisticsDocument81 pagesBasic BioostatisticsCandace Wilson ghNo ratings yet
- Social and Preventive MedicineDocument94 pagesSocial and Preventive MedicineRazor GGNo ratings yet
- Epidemiology Practice Exam Answers FallDocument20 pagesEpidemiology Practice Exam Answers Fallpmp123456No ratings yet
- II. Natural History of A DiseaseDocument36 pagesII. Natural History of A DiseaseJeffrey Ramos100% (1)
- Relative Risk:: Primary Disease Is More Common in A Coal WorkerDocument2 pagesRelative Risk:: Primary Disease Is More Common in A Coal WorkerCompilation MasterNo ratings yet
- Bias and ConfoundingDocument27 pagesBias and ConfoundingsanjivdasNo ratings yet
- Experimental Design in Clinical TrialsDocument18 pagesExperimental Design in Clinical Trialsarun_azamNo ratings yet
- Epidemiology Lecture NotesDocument178 pagesEpidemiology Lecture NotesImtiaz Husain83% (6)
- Analytical EpidemiologyDocument28 pagesAnalytical EpidemiologyZuha HundalNo ratings yet
- Overview of Epidemiological Study DesignsDocument16 pagesOverview of Epidemiological Study DesignsLakshmi Seth100% (2)
- Epi Exam 2 Q&aDocument13 pagesEpi Exam 2 Q&aeman100% (1)
- Chapter 1 Introduction The Teaching of Theory (3 Hours) ObjectiveDocument32 pagesChapter 1 Introduction The Teaching of Theory (3 Hours) Objectiveapi-3728690100% (1)
- Biostatistics:Descriptive StatisticsDocument146 pagesBiostatistics:Descriptive StatisticsMinlik-alew DejenieNo ratings yet
- Epidemiology Exam Questions and AnswersDocument107 pagesEpidemiology Exam Questions and AnswersilerioluwaibitoyeNo ratings yet
- Preparatory Lecture: Confounding and BiasDocument144 pagesPreparatory Lecture: Confounding and BiasSaeed Al-YafeiNo ratings yet
- Community MCQDocument271 pagesCommunity MCQمحسن حدوان عليخان0% (1)
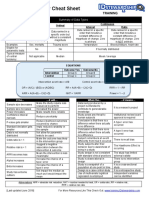
- Biostatistics Study Cheat SheetDocument1 pageBiostatistics Study Cheat Sheetab100% (1)
- Epidemiology Review QuestionsDocument12 pagesEpidemiology Review Questionsdrnzyme100% (6)
- Multiple Choice Questions2 23may2011Document4 pagesMultiple Choice Questions2 23may2011AhmedStatistics40% (5)
- Recommendations for Biostatisticians in Managing and Conducting Medical Research ConsultationsFrom EverandRecommendations for Biostatisticians in Managing and Conducting Medical Research ConsultationsNo ratings yet
- Study Questions EpidemiologyDocument13 pagesStudy Questions Epidemiologythechickendidwhat33% (3)
- Disease Detectives II Host Agent EnvironmentDocument48 pagesDisease Detectives II Host Agent EnvironmentStella Jeong100% (1)
- Tentamen Intro EpiDocument10 pagesTentamen Intro EpiAhmedStatisticsNo ratings yet
- Introduction of Public Health Nursing: Mr. Kailash NagarDocument37 pagesIntroduction of Public Health Nursing: Mr. Kailash NagarKailash NagarNo ratings yet
- Clinical Study: Design and Methods: Hail M. Al-Abdely, MDDocument64 pagesClinical Study: Design and Methods: Hail M. Al-Abdely, MDkazugawaNo ratings yet
- EpidemiologyDocument33 pagesEpidemiologyBheru Lal100% (2)
- Biostats NotesDocument82 pagesBiostats NotesHaroonNo ratings yet
- Epidemiologi Prof Bhisma MurtiDocument32 pagesEpidemiologi Prof Bhisma MurtiniaasetaNo ratings yet
- Variables: Mesfin Kote (BSC., MPHDocument28 pagesVariables: Mesfin Kote (BSC., MPHBetii ManduNo ratings yet
- Lect 2 Research Methods and Study DesignDocument75 pagesLect 2 Research Methods and Study DesignBetii Mandu100% (2)
- 1-Factorial Experiments PDFDocument14 pages1-Factorial Experiments PDFVikki NandeshwarNo ratings yet
- I-Exposure by Island Hospital - Volume 17Document24 pagesI-Exposure by Island Hospital - Volume 17Island HospitalNo ratings yet
- 22 Non-Negotiable Laws of Wellness DiscussionDocument81 pages22 Non-Negotiable Laws of Wellness DiscussionMark Joel Ragndan DulayNo ratings yet
- Health Benefits of Nuts and Dried FruitsDocument557 pagesHealth Benefits of Nuts and Dried FruitsvicNo ratings yet
- Pioneered Products of Sabinsa - Sep 16, 2011Document95 pagesPioneered Products of Sabinsa - Sep 16, 2011ameers333No ratings yet
- Every Child Matters Outcomes FrameworkDocument1 pageEvery Child Matters Outcomes Frameworkapi-16263107No ratings yet
- Health Benefit Application of Functional Oligosaccharides PDFDocument7 pagesHealth Benefit Application of Functional Oligosaccharides PDFmilu1312No ratings yet
- PPS Lab Problem Statements With Write-Up FormatDocument11 pagesPPS Lab Problem Statements With Write-Up FormatSagabh KushhNo ratings yet
- E-Book Vegan FitnessDocument92 pagesE-Book Vegan FitnessMarian Sava100% (4)
- Meal Planning As A Strategy To Support Healthy EatingDocument6 pagesMeal Planning As A Strategy To Support Healthy Eatingnidhi bundhooNo ratings yet
- Ayush TrainingDocument71 pagesAyush Trainingapi-3711488No ratings yet
- Unit 9: Global Epidemic: Causes of ObesityDocument3 pagesUnit 9: Global Epidemic: Causes of ObesityNguyen Hoai ThuongNo ratings yet
- Graded Task 2 - Fitness PlanDocument4 pagesGraded Task 2 - Fitness PlanMa Andrea TabiosNo ratings yet
- Medical Field ThesisDocument7 pagesMedical Field Thesisnicolegomezlittlerock100% (2)
- You Are Not Addicted To Cigarette Smoking You Are Starving: How The Magic Mineral Prevents The Desire To Smoke Chapter 2Document21 pagesYou Are Not Addicted To Cigarette Smoking You Are Starving: How The Magic Mineral Prevents The Desire To Smoke Chapter 2tshkrel100% (2)
- New Microsoft Office Word DocumentDocument102 pagesNew Microsoft Office Word DocumentResearch Center for Training and DevelopmentNo ratings yet
- Group Mediclaim Insurance Policy: 1. ObjectiveDocument11 pagesGroup Mediclaim Insurance Policy: 1. ObjectivesukanyaNo ratings yet
- Health ConsciousDocument28 pagesHealth ConsciousNelson VegaNo ratings yet
- Years of Democracy: Growing South Africa Together For Women's EmancipationDocument26 pagesYears of Democracy: Growing South Africa Together For Women's EmancipationAli AbbasNo ratings yet
- Pe and Health Mod 1Document9 pagesPe and Health Mod 1Krismark IsraelNo ratings yet
- Knapen 2014 Disabil Rehabil ExercisetherapyimprovesbothmentalandphysicalhealthinpatientswithmajordepressionDocument7 pagesKnapen 2014 Disabil Rehabil ExercisetherapyimprovesbothmentalandphysicalhealthinpatientswithmajordepressionShweta KateNo ratings yet
- CBSe English SA2Document6 pagesCBSe English SA2Manoj TyagiNo ratings yet
- ES5101 Week 3 Tutorial Notes Critique WritingDocument11 pagesES5101 Week 3 Tutorial Notes Critique Writingkoksoon chongNo ratings yet
- BMI Classification WhoDocument1 pageBMI Classification WhoMuhammad AkrimNo ratings yet
- Engish 1201 Literary ReviewDocument4 pagesEngish 1201 Literary Reviewapi-509691745No ratings yet
- New Dietary Supplements For Obesity What We Currently KnowDocument9 pagesNew Dietary Supplements For Obesity What We Currently KnowarmandoNo ratings yet
- Exercise Science PhilosophyDocument4 pagesExercise Science Philosophyapi-301109134No ratings yet
- Perdev q1 Mod3 Why Am I Like ThisDocument35 pagesPerdev q1 Mod3 Why Am I Like ThisKenneth MarianoNo ratings yet
- What Doctors Dont Tell You - Your Exercise PlanDocument22 pagesWhat Doctors Dont Tell You - Your Exercise PlanmonteveranoNo ratings yet
- مرجع الفصال العظميDocument7 pagesمرجع الفصال العظميMouhammed SleiayNo ratings yet
- Minkler - Personal Responsibility For HealthDocument22 pagesMinkler - Personal Responsibility For HealthColesniuc Adina100% (1)