You might also like
- Blood Bank TypingDocument34 pagesBlood Bank TypingSkylarNo ratings yet
- B Blab 7 Panel Spring 2012Document16 pagesB Blab 7 Panel Spring 2012pzaballero7063No ratings yet
- 68th AACC Annual Scientific Meeting Abstract eBookFrom Everand68th AACC Annual Scientific Meeting Abstract eBookNo ratings yet
- ImmunoassayDocument7 pagesImmunoassaySanthosh PNo ratings yet
- Detection of AntibodiesDocument7 pagesDetection of AntibodiesJezreeljeanne Largo CaparosoNo ratings yet
- Lesson 07 PDFDocument14 pagesLesson 07 PDFIhsan UllahNo ratings yet
- Lesson 5: Nature of The Clinical LaboratoryDocument8 pagesLesson 5: Nature of The Clinical LaboratoryJohn Daniel AriasNo ratings yet
- (MID) IMMUNOSERO - Chapter 10 - Labeled ImmunoassaysDocument4 pages(MID) IMMUNOSERO - Chapter 10 - Labeled ImmunoassaysAisle Malibiran PalerNo ratings yet
- Gel TechnologyDocument2 pagesGel TechnologyJai Carungay100% (1)
- Latex Agglutination TestDocument2 pagesLatex Agglutination TestIrvy Eleanor Joannes100% (1)
- Non Protein CompoundsDocument64 pagesNon Protein CompoundsAbigail Mayled LausNo ratings yet
- Principles of Serodiagnosis: Ms. Piyumali Arachchi Mphil (Usjp) BSC (Uoc)Document26 pagesPrinciples of Serodiagnosis: Ms. Piyumali Arachchi Mphil (Usjp) BSC (Uoc)Nipun ShamikaNo ratings yet
- Coagulation NotesDocument14 pagesCoagulation NotesthrowawyNo ratings yet
- Assessment and Management of Patients With Hematologic DisordersDocument20 pagesAssessment and Management of Patients With Hematologic Disorderschristine mercado100% (1)
- Abs Elu HandoutDocument6 pagesAbs Elu HandoutSiti Fadhilla TsabithaNo ratings yet
- BOMBAY Blood GroupDocument14 pagesBOMBAY Blood Groupmail2jackal0% (1)
- Exercise 8 Direct Antiglobulin Test (DAT) : ObjectivesDocument9 pagesExercise 8 Direct Antiglobulin Test (DAT) : ObjectivesTrang HuynhNo ratings yet
- Antibody ScreeningDocument57 pagesAntibody ScreeningSebastian Jake John100% (1)
- New Microsoft Word DocumentDocument7 pagesNew Microsoft Word DocumentDocAxi Maximo Jr AxibalNo ratings yet
- Labeled ImmunoassayDocument33 pagesLabeled ImmunoassayCharmeigne Caronan100% (1)
- Antigenandantibodyreaction 120515041533 Phpapp01Document44 pagesAntigenandantibodyreaction 120515041533 Phpapp01Azhar Clinical Laboratory TubeNo ratings yet
- 1 Edited My Class Note 1 On Blood BankDocument42 pages1 Edited My Class Note 1 On Blood Bankmatewos100% (1)
- Introduction To ImmunoassaysDocument45 pagesIntroduction To ImmunoassaysBilla KhanNo ratings yet
- Introduction To ImmunoassaysDocument44 pagesIntroduction To Immunoassaysvidhi100% (1)
- 2.5 Antibody ScreeningDocument5 pages2.5 Antibody ScreeningBALAJINo ratings yet
- Therapeutic Drug MonitoringDocument8 pagesTherapeutic Drug MonitoringLourdette TorrefielNo ratings yet
- Blood BankingDocument7 pagesBlood BankingRoiland Atienza BaybayonNo ratings yet
- Blood BankDocument32 pagesBlood Bankpikachu100% (1)
- Physical Examination of UrineDocument4 pagesPhysical Examination of UrineIceNo ratings yet
- Methods of Hormone AnalysisDocument23 pagesMethods of Hormone AnalysisKumar SaketNo ratings yet
- CH 6 The ABO Blood Group SystemDocument3 pagesCH 6 The ABO Blood Group SystemDixie DumagpiNo ratings yet
- Blood Bank (2 Week) : Antibody ScreensDocument5 pagesBlood Bank (2 Week) : Antibody ScreensAngela ReyesNo ratings yet
- Anti-Globulin Test AGT (Coomb's Test) Direct, IndirectDocument26 pagesAnti-Globulin Test AGT (Coomb's Test) Direct, Indirectlubna aloshibiNo ratings yet
- (CC) Case Study 1 and 2Document11 pages(CC) Case Study 1 and 2Alyssa Nicole BarrettoNo ratings yet
- ABO Blood Group DiscrepanciesDocument9 pagesABO Blood Group DiscrepanciesRichard SiahaanNo ratings yet
- Hormones AnalysisDocument41 pagesHormones AnalysisSULEIMAN OMAR100% (5)
- 2210 ABO Worksheet-1Document3 pages2210 ABO Worksheet-1Lida LindstromNo ratings yet
- Microbiology 15 Campylobacter, Vibrio Etc 431-449Document18 pagesMicrobiology 15 Campylobacter, Vibrio Etc 431-449JenNo ratings yet
- Principles of Immunochemical Techniques PDFDocument8 pagesPrinciples of Immunochemical Techniques PDFdatitoxNo ratings yet
- Alloimmunisation To Blood Group AntigensDocument34 pagesAlloimmunisation To Blood Group AntigensbloodbankNo ratings yet
- Tests For Dengue GROUP 3Document22 pagesTests For Dengue GROUP 3chocoholic potchiNo ratings yet
- Blood Banking Lab Manual 3rdDocument7 pagesBlood Banking Lab Manual 3rdDanna Angelick ReyesNo ratings yet
- HEMOSTASIS Coagulation PathwayDocument3 pagesHEMOSTASIS Coagulation PathwayGianna SablanNo ratings yet
- Urinalysis and Body Fluids2020Document47 pagesUrinalysis and Body Fluids2020MONFOLA100% (1)
- Monoclonal Antibody: Engineering and TherapyDocument39 pagesMonoclonal Antibody: Engineering and TherapyAugusta Rizki AnandaNo ratings yet
- Adverse Reaction Blood BankDocument10 pagesAdverse Reaction Blood BankyourfamilydoctorNo ratings yet
- Elisa & RiaDocument4 pagesElisa & Riadihajum3No ratings yet
- Iron Kinetics and Laboratory AssessmentDocument4 pagesIron Kinetics and Laboratory AssessmentJohnree A. EvangelistaNo ratings yet
- ImmunohematologyDocument4 pagesImmunohematologyosama1381971No ratings yet
- Resolution of Abo DiscrepanciesDocument4 pagesResolution of Abo DiscrepanciesPatrick MabugatNo ratings yet
- Chapter 14 - Routine and Point of Care Testing in HematologyDocument10 pagesChapter 14 - Routine and Point of Care Testing in HematologyNathaniel Sim100% (1)
- Hematology 2 Topic 2 Prelim2222Document73 pagesHematology 2 Topic 2 Prelim2222Mary Lyka ReyesNo ratings yet
- Blood GroupingDocument3 pagesBlood GroupingJalajarani AridassNo ratings yet
- Label ImmunoassayDocument92 pagesLabel ImmunoassayCherry Reyes-Principe100% (3)
- Recall 1Document4 pagesRecall 1pikachuNo ratings yet
- HemaDocument59 pagesHemaSteph VeeNo ratings yet
- Treating SepsisDocument4 pagesTreating SepsisEdwin ClNo ratings yet
- SSC - FCI - Paper Held 5 Feb 2012 Second Sitting 2 PDFDocument22 pagesSSC - FCI - Paper Held 5 Feb 2012 Second Sitting 2 PDFAvi VermaNo ratings yet
- AnaemiaDocument49 pagesAnaemiaAvi VermaNo ratings yet
- Notification of PgiDocument1 pageNotification of PgiAvi VermaNo ratings yet
- Waterhouse-Friderichsen Syndrome NEJMDocument1 pageWaterhouse-Friderichsen Syndrome NEJMAvi VermaNo ratings yet
- Wounds Tissues Aspirates Culture Manual MT - SINAI PDFDocument53 pagesWounds Tissues Aspirates Culture Manual MT - SINAI PDFAvi VermaNo ratings yet
- Urine Culture Manual MT - SINAI PDFDocument15 pagesUrine Culture Manual MT - SINAI PDFAvi VermaNo ratings yet
- AnthraxDocument12 pagesAnthraxAvi Verma100% (1)
- Compatibility Testing For Blood TransfusionDocument51 pagesCompatibility Testing For Blood TransfusiontaecyzNo ratings yet
- Laboratory Methods For The Diagnosis of Epidemic Dysentery and CholeraDocument115 pagesLaboratory Methods For The Diagnosis of Epidemic Dysentery and CholeraCesar AlegreNo ratings yet
- 086 Answer Key Upsc Preliminary Exam (25.05.13)Document2 pages086 Answer Key Upsc Preliminary Exam (25.05.13)Avi VermaNo ratings yet
- Blood Culture Manual MT - SinaiDocument41 pagesBlood Culture Manual MT - SinaiAvi Verma100% (1)
- Chronic Diarrhea NEJM 95Document5 pagesChronic Diarrhea NEJM 95Avi VermaNo ratings yet
- Chronic Diarrhea NEJM 95Document5 pagesChronic Diarrhea NEJM 95Avi VermaNo ratings yet
- B. AnthracisDocument1 pageB. AnthracisAvi VermaNo ratings yet
- NOTESDocument1 pageNOTESAvi VermaNo ratings yet
- Iron Deficiency AnemiaDocument1 pageIron Deficiency AnemiaFrancis Lloyd NeriNo ratings yet
- L E CellDocument59 pagesL E CellAvi VermaNo ratings yet
- Tubular Function TestDocument12 pagesTubular Function TestAvi Verma100% (1)
- CalculiDocument22 pagesCalculiAvi VermaNo ratings yet
- Major Crossmatch Versus TypeScreenDocument13 pagesMajor Crossmatch Versus TypeScreenAvi VermaNo ratings yet
- Major Crossmatch Versus TypeScreenDocument13 pagesMajor Crossmatch Versus TypeScreenAvi VermaNo ratings yet
- Tuberculosis: Presenter - Poonam BSC MLT 3 Year. Moderator-Dr - Neelam KaisthaDocument39 pagesTuberculosis: Presenter - Poonam BSC MLT 3 Year. Moderator-Dr - Neelam KaisthaAvi VermaNo ratings yet
- ColorimeterDocument7 pagesColorimeterAvi VermaNo ratings yet
- Plasma Hemoglobin and Urine Hemoglobin EstimationDocument12 pagesPlasma Hemoglobin and Urine Hemoglobin EstimationAvi VermaNo ratings yet
- Transfusion Reaction - Rachel-La-CountDocument23 pagesTransfusion Reaction - Rachel-La-CountMunish DograNo ratings yet
- Proxymal Nocturnal Haemoglobinuria (PNH)Document39 pagesProxymal Nocturnal Haemoglobinuria (PNH)Avi VermaNo ratings yet
- Microbio Lec 5 - StaphylococcusDocument6 pagesMicrobio Lec 5 - Staphylococcusapi-3743217100% (2)
- Carbohydrate ChemistryDocument14 pagesCarbohydrate ChemistryAvi VermaNo ratings yet
- Urinary Tract Infection: Presented by - Reeta Sharma Moderator-Dr. ....Document23 pagesUrinary Tract Infection: Presented by - Reeta Sharma Moderator-Dr. ....Avi VermaNo ratings yet
- Algoritma Penanganan Kejang AkutDocument1 pageAlgoritma Penanganan Kejang AkutEwa ClaudiaNo ratings yet
- Articulo Farmacologia PDFDocument4 pagesArticulo Farmacologia PDFMichelle RojoNo ratings yet
- Chapter 42 - Upper Urinary Tract: TraumaDocument2 pagesChapter 42 - Upper Urinary Tract: TraumaSyahdat NurkholiqNo ratings yet
- FHSISDocument15 pagesFHSISThon Lopez MagpantayNo ratings yet
- GE Versana Balance Platinum BrosjyreDocument8 pagesGE Versana Balance Platinum BrosjyreRicky ImranNo ratings yet
- Acute Renal FailureDocument1 pageAcute Renal FailureSonia Letran Singson100% (1)
- Prenatal and Postpartum Aromatherapy ResourcesDocument2 pagesPrenatal and Postpartum Aromatherapy Resourcescansu sezerNo ratings yet
- Surgery 37: Recent Advances inDocument226 pagesSurgery 37: Recent Advances inmudasir61No ratings yet
- MCI One Pager Version 1.0 Oct 2020Document1 pageMCI One Pager Version 1.0 Oct 2020naval730107No ratings yet
- 5 Times Sit To Stand TestDocument7 pages5 Times Sit To Stand TestMelany PenagosNo ratings yet
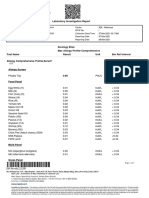
- Laboratory Investigation ReportDocument7 pagesLaboratory Investigation ReportAmarjeetNo ratings yet
- International Wound Journal Volume 7 Issue 4 2010 (Doi 10.1111/j.1742-481x.2010.00682.x) Christine A Chrisman - Care of Chronic Wounds in Palliative Care and End-Of-Life Patients PDFDocument22 pagesInternational Wound Journal Volume 7 Issue 4 2010 (Doi 10.1111/j.1742-481x.2010.00682.x) Christine A Chrisman - Care of Chronic Wounds in Palliative Care and End-Of-Life Patients PDFNovaNo ratings yet
- Quitnet Presentation-Csu StanislausDocument14 pagesQuitnet Presentation-Csu StanislausMaria Carmela CabalquintoNo ratings yet
- Aspirin Paracetamol CaffeineDocument3 pagesAspirin Paracetamol CaffeineMariusNeicuNo ratings yet
- Approach To Nursing Assessment 1Document5 pagesApproach To Nursing Assessment 1Taiye OkondoNo ratings yet
- Astrazenica 2nd Dose 8-13-21 AlkieDocument109 pagesAstrazenica 2nd Dose 8-13-21 AlkieGanie Mar BiasonNo ratings yet
- Chronic MegacolonDocument3 pagesChronic Megacolondrnareshkumar3281No ratings yet
- Womens Knowledge Regarding Symptoms of Menopause in Al Najaf CityDocument9 pagesWomens Knowledge Regarding Symptoms of Menopause in Al Najaf CityakankshaNo ratings yet
- Hip Resurfacing Expectations and LimitationsDocument4 pagesHip Resurfacing Expectations and LimitationsCristian BenayNo ratings yet
- Home Study Course-HomeopathDocument155 pagesHome Study Course-HomeopathAzad Ansari67% (6)
- Sarcomas of The Head and Neck: Dr. DarwitoDocument60 pagesSarcomas of The Head and Neck: Dr. DarwitolaurasheerNo ratings yet
- Archaeus 4Document107 pagesArchaeus 4terrythecensorNo ratings yet
- Slow Contact Tracing' Blamed For Spread of New CoronavirusDocument6 pagesSlow Contact Tracing' Blamed For Spread of New CoronavirusProdigal RanNo ratings yet
- Rachael Stanton Resume Rachael Stanton LVT 1 2Document2 pagesRachael Stanton Resume Rachael Stanton LVT 1 2api-686124613No ratings yet
- Nursing Care Plans - Nursing Dia - Gulanick, MegDocument1,374 pagesNursing Care Plans - Nursing Dia - Gulanick, Megeric parl91% (22)
- News 638228866844085591Document4 pagesNews 638228866844085591Divya Prakash KushwahaNo ratings yet
- Question 1Document87 pagesQuestion 1hemihemaNo ratings yet
- HSG Maxessential Brochure W ForeignersDocument18 pagesHSG Maxessential Brochure W Foreignersswapnil.pandeyNo ratings yet
- Crowd Management PolicyDocument3 pagesCrowd Management PolicyAffan sami rayeenNo ratings yet
- Dr. Manella Joseph Senior Lecturer/Consultant PathologistDocument41 pagesDr. Manella Joseph Senior Lecturer/Consultant PathologistNipun Shamika100% (1)