You might also like
- Aortic Stenosis, Mitral Regurgitation, Pulmonary Stenosis, and Tricuspid Regurgitation: Causes, Symptoms, Signs, and TreatmentDocument7 pagesAortic Stenosis, Mitral Regurgitation, Pulmonary Stenosis, and Tricuspid Regurgitation: Causes, Symptoms, Signs, and TreatmentChuu Suen TayNo ratings yet
- Space DynamicsDocument37 pagesSpace Dynamicspurushottam KashyapNo ratings yet
- Theoretical and Actual CombustionDocument14 pagesTheoretical and Actual CombustionErma Sulistyo R100% (1)
- Man Instructions PDFDocument4 pagesMan Instructions PDFAleksandar NikolovskiNo ratings yet
- Project On Stones & TilesDocument41 pagesProject On Stones & TilesMegha GolaNo ratings yet
- Complications of PuerperiumDocument45 pagesComplications of PuerperiumsubashikNo ratings yet
- CP 343-1Document23 pagesCP 343-1Yahya AdamNo ratings yet
- Seminar On Complication of 3rd Stage PPHDocument13 pagesSeminar On Complication of 3rd Stage PPHjuhi labana0% (1)
- Artifact and Thingamy by David MitchellDocument8 pagesArtifact and Thingamy by David MitchellPedro PriorNo ratings yet
- LTE EPC Technical OverviewDocument320 pagesLTE EPC Technical OverviewCristian GuleiNo ratings yet
- Interactive Architecture Adaptive WorldDocument177 pagesInteractive Architecture Adaptive Worldhoma massihaNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- 9600 DocumentDocument174 pages9600 Documentthom38% (13)
- AedaDocument3 pagesAedaFebey Arie MulyaNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument4 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyFebrinata MahadikaNo ratings yet
- Paper AbdAllah RefaatDocument13 pagesPaper AbdAllah RefaatAbdAllah A. RefaatNo ratings yet
- Identification of Antiviral Antihistamines For COVID-19 RepurposingDocument6 pagesIdentification of Antiviral Antihistamines For COVID-19 RepurposingAnna JuniedNo ratings yet
- Uterine AtonyDocument4 pagesUterine AtonyJohn Cenas100% (1)
- Research ArticleDocument7 pagesResearch ArticleHazbullah AisyNo ratings yet
- Fix Tamponed Ballon 3Document8 pagesFix Tamponed Ballon 3Maulana HamzahNo ratings yet
- Safety of Umbilical Cord Milking in Very Preterm Neonates: A Randomized Controlled StudyDocument8 pagesSafety of Umbilical Cord Milking in Very Preterm Neonates: A Randomized Controlled StudyFatma ElzaytNo ratings yet
- Conservative Management of Placenta Accreta in A Multiparous WomanDocument10 pagesConservative Management of Placenta Accreta in A Multiparous WomanRobel Mae Lagos MontañoNo ratings yet
- The Hayman TechniqueDocument4 pagesThe Hayman TechniquejaulloqueNo ratings yet
- Bakri BalloonDocument3 pagesBakri BalloonancoursNo ratings yet
- A Safe and Effective Method of ControllingDocument3 pagesA Safe and Effective Method of Controllingelizabeth2112No ratings yet
- Evidence of Self-Directed Learning: 1. Reflection On Ectopic Pregnancy RetrievedDocument3 pagesEvidence of Self-Directed Learning: 1. Reflection On Ectopic Pregnancy RetrievedJasha MaeNo ratings yet
- Acquired Hemophilia As A Cause of Primary Postpartum HemorrhageDocument4 pagesAcquired Hemophilia As A Cause of Primary Postpartum HemorrhagedrpiratheepanNo ratings yet
- Management of Postpartum Haemorrhage GuidelineDocument9 pagesManagement of Postpartum Haemorrhage GuidelineAyman A ArafatNo ratings yet
- Success Factors For Bakri Balloon Usage Secondary To Uterine Atony: A Retrospective, Multicentre StudyDocument6 pagesSuccess Factors For Bakri Balloon Usage Secondary To Uterine Atony: A Retrospective, Multicentre StudyMajo MelchiadeNo ratings yet
- Surgical Methods of MTPDocument44 pagesSurgical Methods of MTPRajeev Sood100% (1)
- What Is The Recurrence Rate of Postmenopausal Bleeding in Women Who Have A Thin Endometrium During A First Episode of Postmenopausal Bleeding?Document6 pagesWhat Is The Recurrence Rate of Postmenopausal Bleeding in Women Who Have A Thin Endometrium During A First Episode of Postmenopausal Bleeding?dwiagusyuliantoNo ratings yet
- Managment of Scar PregnancyDocument43 pagesManagment of Scar Pregnancyvacha sardarNo ratings yet
- Normal Vaginal Delivery After One Lower Segment Caesarean Section Can Be Safe Option For Many Women But Not Right Choice For AllDocument6 pagesNormal Vaginal Delivery After One Lower Segment Caesarean Section Can Be Safe Option For Many Women But Not Right Choice For AllRussel Cauton de JesusNo ratings yet
- Cesarean Scar Pregnancy: Some Management OptionsDocument4 pagesCesarean Scar Pregnancy: Some Management OptionsFerro PratamaNo ratings yet
- PP Hemhorrage ArticleDocument6 pagesPP Hemhorrage Articleapi-316491996No ratings yet
- New Options for Managing Adherent PlacentaDocument6 pagesNew Options for Managing Adherent PlacentaAngelique Ramos PascuaNo ratings yet
- Talc Pleurodesis Through Indwelling Pleural Catheters For Malignant Pleural Effusions Retrospective Case Series of A Novel Clinical PathwayDocument5 pagesTalc Pleurodesis Through Indwelling Pleural Catheters For Malignant Pleural Effusions Retrospective Case Series of A Novel Clinical PathwayRosmadi IsmailNo ratings yet
- Day Case Vaginal Pomeroy Tubectomy A Simplified TechniqueDocument11 pagesDay Case Vaginal Pomeroy Tubectomy A Simplified TechniqueedelinNo ratings yet
- Management of Anembryonic Pregnancy Loss: An Observational StudyDocument6 pagesManagement of Anembryonic Pregnancy Loss: An Observational StudyAnonymous ORleRrNo ratings yet
- Case ReportDocument5 pagesCase ReportMira WardhaniNo ratings yet
- Jurnal 1Document10 pagesJurnal 1Ismail RasminNo ratings yet
- Uog 14728Document25 pagesUog 14728Stanley PhanNo ratings yet
- Maternal and Fetal Outcome in Emergency Caesarean Sections in Wad Medani Obstetrics and Gynaecology Hospital Gezira State-SudanDocument12 pagesMaternal and Fetal Outcome in Emergency Caesarean Sections in Wad Medani Obstetrics and Gynaecology Hospital Gezira State-SudanIJAR JOURNALNo ratings yet
- Hydrostatic Reduction of Intussusception in Children - A Single Centre ExperienceDocument9 pagesHydrostatic Reduction of Intussusception in Children - A Single Centre ExperienceMostafa MosbehNo ratings yet
- A Case of Postpartum Hemorrhage Due To Placenta Accreta Diagnosed by Anatomopathology ExamDocument4 pagesA Case of Postpartum Hemorrhage Due To Placenta Accreta Diagnosed by Anatomopathology ExamIJAR JOURNALNo ratings yet
- Hysterosalpingography 2009Document7 pagesHysterosalpingography 2009Niko MontgomeryNo ratings yet
- JurnalDocument7 pagesJurnalDheaNo ratings yet
- A New Facilitating Technique For Postpartum Hysterectomy at Full Dilatation: Cervical ClampDocument4 pagesA New Facilitating Technique For Postpartum Hysterectomy at Full Dilatation: Cervical ClampJani SheNo ratings yet
- Management of Acute Cholecystitis in UK Hospitals: Time For A ChangeDocument4 pagesManagement of Acute Cholecystitis in UK Hospitals: Time For A ChangeRana BishwoNo ratings yet
- Journal Pone 0105882Document7 pagesJournal Pone 0105882Ayu Wedhani SpcNo ratings yet
- Journal Gyn KETDocument8 pagesJournal Gyn KETImaylani S. SitanggangNo ratings yet
- Therapeutic efficacy of hysterosalpingography with hydrostatic pressureDocument5 pagesTherapeutic efficacy of hysterosalpingography with hydrostatic pressurefishalNo ratings yet
- Outcome of Total Laparoscopic HysterectomyDocument4 pagesOutcome of Total Laparoscopic HysterectomyDanica SavićNo ratings yet
- CORDOCENTESISDocument4 pagesCORDOCENTESISDaily DoseNo ratings yet
- Post Partum Hemorrhage Causes and ManagementDocument5 pagesPost Partum Hemorrhage Causes and ManagementLorenn AdarnaNo ratings yet
- Um - Haemorrhage/cd001337 - Diazv - Com/en/: SumberDocument4 pagesUm - Haemorrhage/cd001337 - Diazv - Com/en/: SumberrifkialbanaNo ratings yet
- Acta Obstet Gynecol Scand - 2012 - AIBAR - Bakri Balloon For The Management of Postpartum HemorrhageDocument3 pagesActa Obstet Gynecol Scand - 2012 - AIBAR - Bakri Balloon For The Management of Postpartum HemorrhageOleinic VeraNo ratings yet
- Presentation 5Document23 pagesPresentation 5pallaviNo ratings yet
- Ojog 2013020415273326Document6 pagesOjog 2013020415273326Achmad Safi'iNo ratings yet
- Medical Abortion Lakeland.20130308.025710Document2 pagesMedical Abortion Lakeland.20130308.025710margin15kittenNo ratings yet
- (1875855X - Asian Biomedicine) Conservative Surgical Management For Immediate Postpartum HemorrhageDocument5 pages(1875855X - Asian Biomedicine) Conservative Surgical Management For Immediate Postpartum HemorrhageRatna LuthfiaNo ratings yet
- Scrotal Migration of The Distal End of The Ventriculoperitoneal Shunt Is There A Role For Early Closure of Patent Processus Vaginalis in The Pediatric PopulationDocument4 pagesScrotal Migration of The Distal End of The Ventriculoperitoneal Shunt Is There A Role For Early Closure of Patent Processus Vaginalis in The Pediatric PopulationAthenaeum Scientific Publishers100% (1)
- Caesarean Section4817080565385082090Document38 pagesCaesarean Section4817080565385082090DoaaNo ratings yet
- "Post Partum Hemorrhage: Causes and Management ": Shortreport Open AccessDocument6 pages"Post Partum Hemorrhage: Causes and Management ": Shortreport Open AccessDimas Gatra DiantoroNo ratings yet
- Post Hysteroscopic Progesterone Hormone Therapy in The Treatment of Endometrial PolypsDocument5 pagesPost Hysteroscopic Progesterone Hormone Therapy in The Treatment of Endometrial PolypsherryNo ratings yet
- A Rare Case of Morbidly Adherent Placenta in A Young - 2024 - International JouDocument4 pagesA Rare Case of Morbidly Adherent Placenta in A Young - 2024 - International JouRonald QuezadaNo ratings yet
- Peripartum Hysterectomy: A Life Saving Procedure: Original ArticleDocument4 pagesPeripartum Hysterectomy: A Life Saving Procedure: Original ArticleEdwin MasholaNo ratings yet
- Burst Abdomen A Post-Operative MorbidityDocument4 pagesBurst Abdomen A Post-Operative MorbidityDian AdiNo ratings yet
- Pi Is 0020729214001040Document5 pagesPi Is 0020729214001040Nurul AiniNo ratings yet
- Rate The Highland 2017Document2 pagesRate The Highland 2017Surya PratamaNo ratings yet
- Monkeypox Outbreak in the USDocument39 pagesMonkeypox Outbreak in the USAnonymous llBSa7No ratings yet
- Drug-induced Liver Disease (DILD) Causes, Types, DiagnosisDocument30 pagesDrug-induced Liver Disease (DILD) Causes, Types, DiagnosisSurya PratamaNo ratings yet
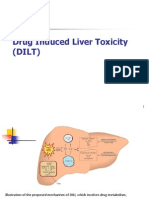
- Drug Induced Liver Toxicity (DILD)Document39 pagesDrug Induced Liver Toxicity (DILD)Surya Pratama100% (1)
- Reducing Risks in Obstetrics & GynecologyDocument30 pagesReducing Risks in Obstetrics & GynecologySurya PratamaNo ratings yet
- HIV/AIDS Teenagers Statistics ProtectionDocument12 pagesHIV/AIDS Teenagers Statistics ProtectionSurya PratamaNo ratings yet
- SleDocument71 pagesSleIrfandy Chairi Sulaiman LubisNo ratings yet
- Acute Viral HepatitisDocument22 pagesAcute Viral HepatitisSurya PratamaNo ratings yet
- 07PHC Book Chapter12Document12 pages07PHC Book Chapter12Surya PratamaNo ratings yet
- Library Dissertation in Community DentistryDocument9 pagesLibrary Dissertation in Community DentistryPayForPaperCanada100% (1)
- Feline DermatologyDocument55 pagesFeline DermatologySilviuNo ratings yet
- Is.4162.1.1985 Graduated PipettesDocument23 pagesIs.4162.1.1985 Graduated PipettesBala MuruNo ratings yet
- Motor Wiring Diagram: D.C. Motor ConnectionsDocument1 pageMotor Wiring Diagram: D.C. Motor Connectionsczds6594No ratings yet
- Telco XPOL MIMO Industrial Class Solid Dish AntennaDocument4 pagesTelco XPOL MIMO Industrial Class Solid Dish AntennaOmar PerezNo ratings yet
- Mechanical Specifications For Fiberbond ProductDocument8 pagesMechanical Specifications For Fiberbond ProducthasnizaNo ratings yet
- Fraktur Dentoalevolar (Yayun)Document22 pagesFraktur Dentoalevolar (Yayun)Gea RahmatNo ratings yet
- Air Wellness QRSDocument2 pagesAir Wellness QRSapi-3743459No ratings yet
- Diia Specification: Dali Part 252 - Energy ReportingDocument15 pagesDiia Specification: Dali Part 252 - Energy Reportingtufta tuftaNo ratings yet
- Peptic Ulcer Disease: Causes, Symptoms and TreatmentDocument24 pagesPeptic Ulcer Disease: Causes, Symptoms and TreatmentOktaviana Sari Dewi100% (1)
- Introduction To Finite Element Methods (2001) (En) (489s)Document489 pagesIntroduction To Finite Element Methods (2001) (En) (489s)green77parkNo ratings yet
- Nickel-Metal Hydride Battery Safety Data SheetDocument8 pagesNickel-Metal Hydride Battery Safety Data SheetYeong WheeNo ratings yet
- Chemistry of FormazanDocument36 pagesChemistry of FormazanEsteban ArayaNo ratings yet
- Motor GraderDocument24 pagesMotor GraderRafael OtuboguatiaNo ratings yet
- JUPITER 9000K H1PreliminaryDocument1 pageJUPITER 9000K H1PreliminaryMarian FlorescuNo ratings yet
- Concept Page - Using Vagrant On Your Personal Computer - Holberton Intranet PDFDocument7 pagesConcept Page - Using Vagrant On Your Personal Computer - Holberton Intranet PDFJeffery James DoeNo ratings yet
- VA TearDownDocument5 pagesVA TearDownfaj_larcfave5149No ratings yet
- Organizing Small Items with Glass Bottle OrganizersDocument70 pagesOrganizing Small Items with Glass Bottle OrganizersDy SaiNo ratings yet
- Taking Back SundayDocument9 pagesTaking Back SundayBlack CrowNo ratings yet
- 40 26Document3 pages40 26Maxi452No ratings yet