You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Anatomy ModelsDocument5 pagesAnatomy ModelstashanabrazhNo ratings yet
- Section 80DD, Section 80DDB, Section 80U - Tax Deduction For Disabled PersonsDocument19 pagesSection 80DD, Section 80DDB, Section 80U - Tax Deduction For Disabled Personsvvijayaraghava100% (1)
- Prostate Massage - Wikipedia, The Free EncyclopediaDocument5 pagesProstate Massage - Wikipedia, The Free EncyclopediaA R KhanNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Label Reproductive Systems - QuestionsDocument5 pagesLabel Reproductive Systems - QuestionsKatieNo ratings yet
- Excretory System - Print - QuizizzDocument4 pagesExcretory System - Print - Quizizzosama0% (1)
- Calcitriol - Drug InformationDocument13 pagesCalcitriol - Drug InformationNikesh DoshiNo ratings yet
- Improved Survival in Patients With End-Stage Cancer Treated With Coenzyme Q10Document13 pagesImproved Survival in Patients With End-Stage Cancer Treated With Coenzyme Q10Nikesh DoshiNo ratings yet
- Uoa Brochure NeobladderDocument2 pagesUoa Brochure NeobladderSaikat Prasad DattaNo ratings yet
- EMS Urology CatalogDocument41 pagesEMS Urology CatalogIon VasianNo ratings yet
- Approach To A Patient With HaematuriaDocument21 pagesApproach To A Patient With HaematuriaMisbah KaleemNo ratings yet
- Chronic Kidney Disease in PregnancyDocument5 pagesChronic Kidney Disease in PregnancyNikesh DoshiNo ratings yet
- Outcome of Pregnancy in Women With Moderate or Severe Renal InsufficiencyDocument7 pagesOutcome of Pregnancy in Women With Moderate or Severe Renal InsufficiencyNikesh DoshiNo ratings yet
- Diabetes Complications Avoidance and ManagementDocument67 pagesDiabetes Complications Avoidance and ManagementNikesh DoshiNo ratings yet
- Calorie Intake and Patient Outcomes in Severe Acute Kidney Injury - DDocument11 pagesCalorie Intake and Patient Outcomes in Severe Acute Kidney Injury - DNikesh DoshiNo ratings yet
- The Status of Synbiotics in Colorectal CancerDocument15 pagesThe Status of Synbiotics in Colorectal CancerNikesh DoshiNo ratings yet
- "Care," Cancer and Coenzyme Q10Document7 pages"Care," Cancer and Coenzyme Q10Nikesh DoshiNo ratings yet
- Potential Role of Probiotics On Colorectal Cancer PreventionDocument8 pagesPotential Role of Probiotics On Colorectal Cancer PreventionNikesh DoshiNo ratings yet
- The Role of Coenzyme Q in Clinical Medicine: Part I: Alan R. Gaby, MDDocument7 pagesThe Role of Coenzyme Q in Clinical Medicine: Part I: Alan R. Gaby, MDAnonymous mKdAfWifNo ratings yet
- Ts-2 Probiotic Potential of Lactic Acid Bacteria Isolated From Fermented Dairy Milks On Antiproliferation of Colon Cancer CellsDocument6 pagesTs-2 Probiotic Potential of Lactic Acid Bacteria Isolated From Fermented Dairy Milks On Antiproliferation of Colon Cancer CellsNikesh DoshiNo ratings yet
- Gut Microbiota and Probiotics - Current Status and Their Role in Cancer TherapeuticsDocument11 pagesGut Microbiota and Probiotics - Current Status and Their Role in Cancer TherapeuticsNikesh DoshiNo ratings yet
- Calcitriol - Pediatric Drug InformationDocument9 pagesCalcitriol - Pediatric Drug InformationNikesh DoshiNo ratings yet
- The Prevalence of Complementary - Alternative Medicine in CancerDocument6 pagesThe Prevalence of Complementary - Alternative Medicine in CancerNikesh DoshiNo ratings yet
- Piperine Derived From Black Pepper Increases The Plasma Levels of Coenzyme Q10 Following Oral SupplementationDocument5 pagesPiperine Derived From Black Pepper Increases The Plasma Levels of Coenzyme Q10 Following Oral SupplementationNikesh DoshiNo ratings yet
- Espf BBS 001Document102 pagesEspf BBS 001Nikesh DoshiNo ratings yet
- Neurogenic Bladder in SCI - Tutorial 2012Document36 pagesNeurogenic Bladder in SCI - Tutorial 2012Nikesh DoshiNo ratings yet
- CoenzymeQ10 Concentrations Breast Cancer PatientsDocument6 pagesCoenzymeQ10 Concentrations Breast Cancer PatientsNikesh DoshiNo ratings yet
- Anti-Infectives & Their Role in Acute Kidney InjuryDocument34 pagesAnti-Infectives & Their Role in Acute Kidney InjuryNikesh DoshiNo ratings yet
- Ashtead University Hospital Acknowledgment LetterDocument1 pageAshtead University Hospital Acknowledgment LetterNikesh DoshiNo ratings yet
- Causes of HyponatremiaDocument21 pagesCauses of HyponatremiaNikesh DoshiNo ratings yet
- Renal DiseaseDocument19 pagesRenal DiseaseNikesh DoshiNo ratings yet
- An Overview of Urodynamic StudiesDocument54 pagesAn Overview of Urodynamic StudiesNikesh Doshi100% (1)
- Summary and Conclusions: Urinary Biomarkers in Experimental DiabetesDocument1 pageSummary and Conclusions: Urinary Biomarkers in Experimental DiabetesNikesh DoshiNo ratings yet
- RAAS CKD ProgressionDocument86 pagesRAAS CKD ProgressionNikesh DoshiNo ratings yet
- Nephrectomy Overview: Causes of Nonfunctional KidneysDocument4 pagesNephrectomy Overview: Causes of Nonfunctional KidneysNikesh DoshiNo ratings yet
- Medical Complications of Renal Transplantation: Thitisak Kitthaweesin, MDDocument112 pagesMedical Complications of Renal Transplantation: Thitisak Kitthaweesin, MDNikesh DoshiNo ratings yet
- Neurogenic BladderDocument68 pagesNeurogenic BladderNikesh DoshiNo ratings yet
- MBA405 10 HandbookDocument55 pagesMBA405 10 HandbookNikesh DoshiNo ratings yet
- Kidney Tubulointerstitial Diseases GuideDocument13 pagesKidney Tubulointerstitial Diseases GuideDani DanyNo ratings yet
- Chapter 24 HomeworkDocument9 pagesChapter 24 HomeworkKvn4N6No ratings yet
- Bladder PDFDocument22 pagesBladder PDFSuci Mega SariNo ratings yet
- Unilateral Multicystic Dysplastic Kidney Long Term OutcomesDocument4 pagesUnilateral Multicystic Dysplastic Kidney Long Term Outcomespubblicita.landi1969No ratings yet
- Hubungan Antara NLR Dan Aki Pada Pasien SepsisDocument4 pagesHubungan Antara NLR Dan Aki Pada Pasien Sepsisdwi widyaNo ratings yet
- Common Ailments of The Urinary SystemDocument3 pagesCommon Ailments of The Urinary SystemMike NunezaNo ratings yet
- Inj 2244166 083Document11 pagesInj 2244166 083Suyat SuyatmiNo ratings yet
- HydronephrosisDocument7 pagesHydronephrosisNaqash NobleNo ratings yet
- 990812 EUS教學 (4) 重點式急診泌尿系統超音波之應用Document77 pages990812 EUS教學 (4) 重點式急診泌尿系統超音波之應用juice119100% (2)
- Management of Patients With Renal DisordersDocument29 pagesManagement of Patients With Renal DisordersokaciaNo ratings yet
- Sistem GenitaliaDocument89 pagesSistem Genitaliaayu juniNo ratings yet
- Urologist, Dr. Natan Davoudzadeh Joins NY HealthDocument3 pagesUrologist, Dr. Natan Davoudzadeh Joins NY HealthPR.comNo ratings yet
- Benign Prostatic HyperplasiaDocument16 pagesBenign Prostatic HyperplasiaJood AL AbriNo ratings yet
- Acute Kidney InjuryDocument17 pagesAcute Kidney InjuryPrecious C. MamaradloNo ratings yet
- The Abington Journal 10-03-2012Document22 pagesThe Abington Journal 10-03-2012The Times LeaderNo ratings yet
- Prostatitis Types, Causes and TreatmentsDocument23 pagesProstatitis Types, Causes and TreatmentsDoha Ebed100% (1)
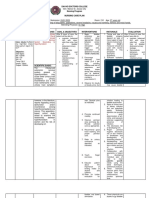
- Davao Doctors College Nursing Program Nursing Care PlanDocument3 pagesDavao Doctors College Nursing Program Nursing Care PlanPRINCESS KOBAYASHINo ratings yet
- UTI, HSC With QuestionsDocument43 pagesUTI, HSC With QuestionsAlex MatthewNo ratings yet
- Bad Sex: Lessons For LifeDocument3 pagesBad Sex: Lessons For Lifestefanaserafina9421No ratings yet
- Record of Terms - February 2018Document78 pagesRecord of Terms - February 2018happyhappylandNo ratings yet
- Aids Education in TanzaniaDocument6 pagesAids Education in TanzaniaSarwin DahNo ratings yet
- Benign Prostatic HyperplasiaDocument5 pagesBenign Prostatic HyperplasiaNimas DwiastutiNo ratings yet