You might also like
- Shock: Dr. Imam Ghozali., Span.,MkesDocument66 pagesShock: Dr. Imam Ghozali., Span.,MkesreavondNo ratings yet
- Shock: Dr. Imam Ghozali., Span.,MkeswDocument70 pagesShock: Dr. Imam Ghozali., Span.,MkeswRiyan SaputraNo ratings yet
- ShockDocument35 pagesShocktrip100No ratings yet
- Shock: Early Reversible and Compensatory ShockDocument6 pagesShock: Early Reversible and Compensatory ShockMaria Ave MariaNo ratings yet
- Circulatory Shock: Santosh DevDocument32 pagesCirculatory Shock: Santosh DevdevdsantoshNo ratings yet
- KP 2.5.5.4 112036 - Shock AlfanDocument52 pagesKP 2.5.5.4 112036 - Shock Alfannurul ramadhiniNo ratings yet
- Shock: Dr. Naser El-Hammuri Head of The Department of Surgery Hashemite UniversityDocument40 pagesShock: Dr. Naser El-Hammuri Head of The Department of Surgery Hashemite UniversityMohammad Husni BanisalmanNo ratings yet
- Lecture Presentation For Clinical 1 StudentsDocument43 pagesLecture Presentation For Clinical 1 Studentskirubel deribNo ratings yet
- Wa0004.Document31 pagesWa0004.Aisha samreenNo ratings yet
- Diagnosis & Treament: ShockDocument52 pagesDiagnosis & Treament: ShockasepNo ratings yet
- Chapter 69Document47 pagesChapter 69Benjamin SchauerteNo ratings yet
- Compensatory Mechanism of Circulatory ShockDocument29 pagesCompensatory Mechanism of Circulatory ShockWan Razin Wan Hassan100% (1)
- ShockDocument52 pagesShockDrSanjeev ShrivastavaNo ratings yet
- Shock - PediaDocument7 pagesShock - PediaCams BonoanNo ratings yet
- Approach to ShockDocument30 pagesApproach to ShocktigistNo ratings yet
- Shock Tugas Anestesi ViliaDocument81 pagesShock Tugas Anestesi ViliaviliaNo ratings yet
- ShockDocument22 pagesShockAbdul MajidNo ratings yet
- Shock & Fluid TherapyDocument57 pagesShock & Fluid Therapyarnol3090No ratings yet
- Biologic CrisisDocument242 pagesBiologic CrisismajNo ratings yet
- Approach To ShockDocument19 pagesApproach To Shocksarath100% (1)
- Diagnosis & Management of Shock: SuriyadiDocument17 pagesDiagnosis & Management of Shock: SuriyadiDeady NurdiantoNo ratings yet
- Shock: Gastrointestinal Surgical Department of Affiliated Hospital of Jining Medical CollegeDocument52 pagesShock: Gastrointestinal Surgical Department of Affiliated Hospital of Jining Medical Collegesanjivdas100% (1)
- Hypovolemic ShockDocument19 pagesHypovolemic ShockJohan BodhiNo ratings yet
- Shock: Departemen Anestesiologi Dan Reanimasi Fakultas Kedokteran USUDocument54 pagesShock: Departemen Anestesiologi Dan Reanimasi Fakultas Kedokteran USURuki HartawanNo ratings yet
- Shock: DR Vishwabharathi TDocument51 pagesShock: DR Vishwabharathi TSumaNo ratings yet
- PBL 1Document111 pagesPBL 1fahmi rosyadiNo ratings yet
- Shock: Aminath Shafa RN MSNDocument30 pagesShock: Aminath Shafa RN MSNMohamed Shuraikh100% (1)
- Shock: Presented By: Robert Siena Eric MacabiogDocument17 pagesShock: Presented By: Robert Siena Eric Macabiogeric macabiogNo ratings yet
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDocument64 pagesShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruNo ratings yet
- Shock FinalDocument90 pagesShock Finalمجاهد إسماعيل حسن حسينNo ratings yet
- PATHOPHYSIOLOGY OF SHOCKDocument56 pagesPATHOPHYSIOLOGY OF SHOCKDr. Haricharan ANo ratings yet
- Penatalaksanaan SyokDocument59 pagesPenatalaksanaan SyokArif NurfadhilahNo ratings yet
- Shock DR Sadia Hussain: Assistant Professor Pediatric Medicine King Edward Medical University LahoreDocument22 pagesShock DR Sadia Hussain: Assistant Professor Pediatric Medicine King Edward Medical University LahoreTouseef Ur RehmanNo ratings yet
- Shock: DR Ahmed MohDocument60 pagesShock: DR Ahmed MohSalman KhanNo ratings yet
- EMS Shock LexDocument60 pagesEMS Shock LexIgor StefanetNo ratings yet
- Shock Syndrome: DR Melkamu BDocument62 pagesShock Syndrome: DR Melkamu BAsteway MesfinNo ratings yet
- Heart FailureDocument4 pagesHeart FailureDane WrightNo ratings yet
- Shock in Children TutorialDocument37 pagesShock in Children TutorialSsenyonga DominicNo ratings yet
- MEDICAL SURGICAL NURSING DISCUSSION ON SHOCKDocument22 pagesMEDICAL SURGICAL NURSING DISCUSSION ON SHOCKNavpreet Kaur100% (1)
- New HeartDocument180 pagesNew HeartivernjayNo ratings yet
- L15-Shock & Resuscitation LectureDocument49 pagesL15-Shock & Resuscitation LectureYosra —No ratings yet
- Hypertension For EMS ProvidersDocument35 pagesHypertension For EMS ProvidersPaulhotvw67100% (5)
- MR Elamin ShockDocument70 pagesMR Elamin ShockMohammed Abd AlgadirNo ratings yet
- Acute Cardiac Crisis: Recognizing Heart FailureDocument77 pagesAcute Cardiac Crisis: Recognizing Heart FailureJudy Anne PatricioNo ratings yet
- ShockDocument19 pagesShockirenekhatete1No ratings yet
- MULTIPLE INJURY SHOCKDocument32 pagesMULTIPLE INJURY SHOCKNazirul HanifNo ratings yet
- Congestive Cardiac FailureDocument49 pagesCongestive Cardiac FailureHampson MalekanoNo ratings yet
- Haemorrhagic Shock, Resuscitation and HaemodynamicsDocument31 pagesHaemorrhagic Shock, Resuscitation and HaemodynamicsNinaNo ratings yet
- Pulmonary EdemaDocument59 pagesPulmonary EdemamaibejoseNo ratings yet
- CardiovascularDocument34 pagesCardiovascularRianna LarezaNo ratings yet
- Shock: DR Uwanuruochi KelechukwuDocument35 pagesShock: DR Uwanuruochi KelechukwuJake MillerNo ratings yet
- Hypovolemic Shock Cardiogenic Shock Obstructive Shock: Prepared By: HO Tiviyah Mentor: DR Tiong Supervisor: DR Tham MinDocument29 pagesHypovolemic Shock Cardiogenic Shock Obstructive Shock: Prepared By: HO Tiviyah Mentor: DR Tiong Supervisor: DR Tham MinTeik Wei TanNo ratings yet
- Presented by Nithish ReddyDocument41 pagesPresented by Nithish ReddyNithish ReddyNo ratings yet
- ShockDocument53 pagesShockHassan Ahmed100% (3)
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Hepatic Encephalopathy: Causes, Tests, and Treatment OptionsFrom EverandHepatic Encephalopathy: Causes, Tests, and Treatment OptionsRating: 3.5 out of 5 stars3.5/5 (2)
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- COVID-19 and Respiratory System DisordersDocument12 pagesCOVID-19 and Respiratory System DisordersMan'SzAr'diAnSyAhNo ratings yet
- Renal MicrocirculationDocument33 pagesRenal MicrocirculationwiamNo ratings yet
- Hemorrhagic Shock and The MicrovasculatureDocument42 pagesHemorrhagic Shock and The MicrovasculatureRaul DoctoNo ratings yet
- NPPE: Negative Pressure Pulmonary EdemaDocument22 pagesNPPE: Negative Pressure Pulmonary EdemaMed Issam MahouachiNo ratings yet
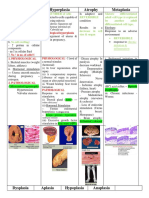
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- Capillary ExchangeDocument27 pagesCapillary Exchangesultan khabeebNo ratings yet
- Eval Microcir Curr - Op.cc 23Document8 pagesEval Microcir Curr - Op.cc 23Julian SanchezNo ratings yet
- Dermatitits StasisDocument11 pagesDermatitits StasisRiyan TjahyaNo ratings yet
- Acute InflammationDocument76 pagesAcute InflammationMuhammad Modu BulamaNo ratings yet
- Pathophysiology of Cardiogenic Pulmonary Edema - UpToDateDocument14 pagesPathophysiology of Cardiogenic Pulmonary Edema - UpToDateStefani AtlleNo ratings yet
- Textbook of Surgery For Dental StudentssDocument399 pagesTextbook of Surgery For Dental StudentssDiana Mihaela Ilie50% (2)
- Shock and Its Nursing InterventionsDocument3 pagesShock and Its Nursing InterventionsWendy EscalanteNo ratings yet
- Arteries & Circulation (Guyton, Chapter 14-16)Document21 pagesArteries & Circulation (Guyton, Chapter 14-16)Dianne IgnacioNo ratings yet
- 56169572-Selected-Readings-in-Plastic-Surgery TextDocument132 pages56169572-Selected-Readings-in-Plastic-Surgery TextyellowbieNo ratings yet
- Cosmetice Celulita PDFDocument4 pagesCosmetice Celulita PDFCarmen Amarandei0% (1)
- Fluid Therapy and The Microcirculation in Health and Critical IllnessDocument11 pagesFluid Therapy and The Microcirculation in Health and Critical IllnessAdote DrmNo ratings yet
- 1 Compression Therapy..Document43 pages1 Compression Therapy..Nermeen7No ratings yet
- The circulatory system - Зүрх судасны тогтолцооDocument2 pagesThe circulatory system - Зүрх судасны тогтолцооKhaliun MyagmarNo ratings yet
- Alfa Tau Herbal Remedies TestimonialDocument55 pagesAlfa Tau Herbal Remedies TestimonialЗорица ЋирићNo ratings yet
- ASEJ D 23 01681 ReviewerDocument12 pagesASEJ D 23 01681 ReviewerKashaf ChNo ratings yet
- 1 s2.0 S0140673622014854 MainDocument12 pages1 s2.0 S0140673622014854 Mainsilvia100% (1)
- Pathophysiology of microcirculation layers and controlDocument37 pagesPathophysiology of microcirculation layers and controlMarina ModringaNo ratings yet
- Boron - Medical PhysiologyDocument13 pagesBoron - Medical PhysiologyOlgaBulat0% (6)
- 001 002 PDFDocument12 pages001 002 PDFalanwalker12thNo ratings yet
- 9D NLBA Illustrated Glossary 2015Document141 pages9D NLBA Illustrated Glossary 2015galante81No ratings yet
- Regulation of Microcirculation and Lymph FlowDocument53 pagesRegulation of Microcirculation and Lymph Flowjulesarojinee100% (2)
- Cerebral Perfusion Simulation Using Realistically Generated Synthetic TreesDocument9 pagesCerebral Perfusion Simulation Using Realistically Generated Synthetic Treessunhao13287710014No ratings yet
- Sindrom Multiple Disfungsi OrganDocument8 pagesSindrom Multiple Disfungsi OrganAdi Nugroho MelyanaNo ratings yet
- Noncardiogenic Pulmonary EdemaDocument12 pagesNoncardiogenic Pulmonary EdemaIrina DuceacNo ratings yet
- Capillaroscopy InfoDocument16 pagesCapillaroscopy InfoAlina BanicaNo ratings yet