You might also like
- Translational Research in Coronary Artery Disease: Pathophysiology to TreatmentFrom EverandTranslational Research in Coronary Artery Disease: Pathophysiology to TreatmentNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Clinical Therapeutics/Volume 39, Number 10, 2017: These Authors Contributed Equally To This WorkDocument12 pagesClinical Therapeutics/Volume 39, Number 10, 2017: These Authors Contributed Equally To This WorkskoamdaskondiajosNo ratings yet
- 2005 ProactiveDocument11 pages2005 ProactiveBanky SupittayapornNo ratings yet
- TopcatDocument11 pagesTopcatLookbua SiraprapaNo ratings yet
- Eci 12025Document11 pagesEci 12025ger4ld1nNo ratings yet
- EBP Article 5Document7 pagesEBP Article 5awuahbohNo ratings yet
- Chronic Kidney DiseaseeGFR RevisedDocument46 pagesChronic Kidney DiseaseeGFR RevisedojannovicNo ratings yet
- The Effect of Cilostazol On Right Heart FunctionDocument43 pagesThe Effect of Cilostazol On Right Heart FunctionGunawan YogaNo ratings yet
- Eplerenone and Atrial Fibrillation in Mild Systolic Heart FailureDocument6 pagesEplerenone and Atrial Fibrillation in Mild Systolic Heart FailureJim Dominguez RosalesNo ratings yet
- Allopurinol and Mortality in Hyperuricaemic Patients: Concise ReportDocument3 pagesAllopurinol and Mortality in Hyperuricaemic Patients: Concise ReporterilarchiNo ratings yet
- Pathophysiology of COPDDocument4 pagesPathophysiology of COPDrinieeeNo ratings yet
- 1.slide Igp Expo Dr. Aulia EditDocument34 pages1.slide Igp Expo Dr. Aulia EditNita Juliana AnggrainiNo ratings yet
- Dia Care-2005-Sever-1151-7Document7 pagesDia Care-2005-Sever-1151-7Barbara Sakura RiawanNo ratings yet
- Ehf2 8 625Document9 pagesEhf2 8 625elza pratiwiNo ratings yet
- Worldwide Trends in Diabetes Since 1980Document484 pagesWorldwide Trends in Diabetes Since 1980L P Lozada MartinezNo ratings yet
- The Effect of Combined Aerobic and Resistance Exercise Training On Vascular Function in Type 2 DiabetesDocument7 pagesThe Effect of Combined Aerobic and Resistance Exercise Training On Vascular Function in Type 2 DiabetesZINATUL WIDADNo ratings yet
- Bi-Preterax Slide Set CI 15 - 16Document35 pagesBi-Preterax Slide Set CI 15 - 16drnasim20088171No ratings yet
- The Perindopril in Elderly PeopleDocument8 pagesThe Perindopril in Elderly PeopleluchititaNo ratings yet
- Mottillo2010 PDFDocument20 pagesMottillo2010 PDFSintia CahyaniNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofGonzalo LealNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofAlina PirtacNo ratings yet
- Bahan Semiloka LitbangDocument15 pagesBahan Semiloka LitbangArumrukmasariNo ratings yet
- Advpub - CJ 15 0702 PDFDocument9 pagesAdvpub - CJ 15 0702 PDFNefri ArshintaNo ratings yet
- Ardsnetwork (Nhlbi) Studies: Successesand Challengesinards ClinicalresearchDocument10 pagesArdsnetwork (Nhlbi) Studies: Successesand Challengesinards ClinicalresearchEduardo SoaresNo ratings yet
- Cardiovascular Risk in Clopidogrel-Treated Patients According To Cytochrome P450 2C19 2 Loss-of-Function Allele or Proton Pump Inhibitor CoadministrationDocument10 pagesCardiovascular Risk in Clopidogrel-Treated Patients According To Cytochrome P450 2C19 2 Loss-of-Function Allele or Proton Pump Inhibitor CoadministrationVenansius ReinaldiNo ratings yet
- How Does Empagliflozin Improve Arterial Stiffness in Patients With Type 2 Diabetes Mellitus - Sub Analysis of A Clinical TrialDocument12 pagesHow Does Empagliflozin Improve Arterial Stiffness in Patients With Type 2 Diabetes Mellitus - Sub Analysis of A Clinical TrialMarshall ThompsonNo ratings yet
- Jurnal SpironolaktonDocument8 pagesJurnal SpironolaktonMedi PutraNo ratings yet
- Clinchem 2013 203778 FullDocument9 pagesClinchem 2013 203778 FullHarnadi WonogiriNo ratings yet
- Jurnal Blok 10Document3 pagesJurnal Blok 10Yunus Lumban RajaNo ratings yet
- Abstracts S257: Ottawa, OntarioDocument2 pagesAbstracts S257: Ottawa, OntarioTrương Công ViệtNo ratings yet
- Nej M 199511163332001Document7 pagesNej M 199511163332001valinttonyNo ratings yet
- Evacetrapib y Resultados Cardiovasculares en La Enfermedad Vascular de Alto RiesgoDocument10 pagesEvacetrapib y Resultados Cardiovasculares en La Enfermedad Vascular de Alto RiesgoAlan Villegas SorianoNo ratings yet
- New England Journal Medicine: The ofDocument12 pagesNew England Journal Medicine: The ofPabellón 4No ratings yet
- American Heart American Heart American Heart American Heart AssociationDocument11 pagesAmerican Heart American Heart American Heart American Heart Associationmubarak19855No ratings yet
- Serum Concentrations of Adiponectin and Risk of Type 2 Diabetes Mellitus and Coronary Heart Disease in Apparently Healthy Middle-Aged MenDocument15 pagesSerum Concentrations of Adiponectin and Risk of Type 2 Diabetes Mellitus and Coronary Heart Disease in Apparently Healthy Middle-Aged MenEcha MagungNo ratings yet
- A Randomized, Double Blind Comparison of Lactated.61Document7 pagesA Randomized, Double Blind Comparison of Lactated.61Temoc TemocNo ratings yet
- Do Angiotensin Converting Enzyme Inhibitors or Angiotensin Receptor Blockers Prevent Diabetes Mellitus? A Meta-AnalysisDocument9 pagesDo Angiotensin Converting Enzyme Inhibitors or Angiotensin Receptor Blockers Prevent Diabetes Mellitus? A Meta-AnalysisURSULA LAZONo ratings yet
- 464 FullDocument11 pages464 FullgunnasundaryNo ratings yet
- Journal Homepage: - : IntroductionDocument3 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Dia Care-2006-Knopp-1478-85Document8 pagesDia Care-2006-Knopp-1478-85Barbara Sakura RiawanNo ratings yet
- Jcu 17 127 PDFDocument8 pagesJcu 17 127 PDFRezkyFYNo ratings yet
- Intraplatelet Serotonin in Patients With Diabetes Mellitus and Peripheral Vascular DiseaseDocument6 pagesIntraplatelet Serotonin in Patients With Diabetes Mellitus and Peripheral Vascular DiseaseHyeon DaNo ratings yet
- Pages From StatinsUpdate-FINALDocument1 pagePages From StatinsUpdate-FINALMuhammad NasrullahNo ratings yet
- Komplikasi Stroke PDFDocument7 pagesKomplikasi Stroke PDFJose Hady PuteraNo ratings yet
- ARB and CCB CombinationDocument11 pagesARB and CCB CombinationLucky PratamaNo ratings yet
- Am J Surg 2004 p463Document4 pagesAm J Surg 2004 p463olivia magdalenaNo ratings yet
- Role of Calcium Channel Antagonism in Vasodilator Effects of 17 - EstradiolDocument5 pagesRole of Calcium Channel Antagonism in Vasodilator Effects of 17 - EstradiolelisasusantiNo ratings yet
- A Randomized Controlled Trial of The Effects of N 3 Fatty Acids On Resolvins in Chronic Kidney Disease - 2016 - Clinical NutritionDocument6 pagesA Randomized Controlled Trial of The Effects of N 3 Fatty Acids On Resolvins in Chronic Kidney Disease - 2016 - Clinical NutritionBby AdelinaNo ratings yet
- PPDS - AT. 28-19 Set K DAFTAR PUSTAKADocument9 pagesPPDS - AT. 28-19 Set K DAFTAR PUSTAKAYeyen amaliahNo ratings yet
- Efficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryDocument9 pagesEfficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryAik NoeraNo ratings yet
- CometDocument9 pagesCometSohail AhmedNo ratings yet
- Lyon Diet Heart Study - de Lorgeril 1994Document6 pagesLyon Diet Heart Study - de Lorgeril 1994acolpoNo ratings yet
- 302 Cardiovascular Risk: AssessmentDocument1 page302 Cardiovascular Risk: AssessmentLêHữuHoàiNo ratings yet
- Crosstalk Between Nafld and CKD and Its Effect On EgfrDocument5 pagesCrosstalk Between Nafld and CKD and Its Effect On EgfrIJAR JOURNALNo ratings yet
- International Journal of Cardiology: Shou-Guo Zhao, Ji-Min Wang, Qian-Feng Han, Tai Li, Heng-Chen YaoDocument2 pagesInternational Journal of Cardiology: Shou-Guo Zhao, Ji-Min Wang, Qian-Feng Han, Tai Li, Heng-Chen YaoMussaNo ratings yet
- ISH/ESH Late-Breaking Trial Results: ANBP2, PHYLLIS, LIFE, ELSA, Eplerenone, STOP-NIDDM, HYVET-Pilot, OCTAVEDocument5 pagesISH/ESH Late-Breaking Trial Results: ANBP2, PHYLLIS, LIFE, ELSA, Eplerenone, STOP-NIDDM, HYVET-Pilot, OCTAVEMihailescu DeeaNo ratings yet
- Diastolic Function Is A Strong Predictor of Mortality in Patients With Chronic Kidney DiseaseDocument6 pagesDiastolic Function Is A Strong Predictor of Mortality in Patients With Chronic Kidney DiseasehanifahrafaNo ratings yet
- Metabolic Cardiovascular Disease Risk Factors and Their Clustering in Subclinical HypothyroidismDocument7 pagesMetabolic Cardiovascular Disease Risk Factors and Their Clustering in Subclinical HypothyroidismMaria Alice BourneufNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- Sexually Transmitted Diseases - CDCDocument116 pagesSexually Transmitted Diseases - CDCAnthony GómezNo ratings yet
- Caduet (Dr. Ismahun Maret 2009)Document41 pagesCaduet (Dr. Ismahun Maret 2009)Yulia SumarnaNo ratings yet
- Molecular and Vascular Evidence in Managing Hypertension and Hyperlipidemia (Dr. Hananto AdriantoDocument77 pagesMolecular and Vascular Evidence in Managing Hypertension and Hyperlipidemia (Dr. Hananto AdriantoYulia SumarnaNo ratings yet
- Endru HartonoDocument3 pagesEndru HartonoYulia SumarnaNo ratings yet
- 1165 Assignment Two Type TwoDocument8 pages1165 Assignment Two Type Twohold00782307No ratings yet
- CPR With AedDocument37 pagesCPR With AedDoc Prince CaballeroNo ratings yet
- Perspective: Plant-Based Eating Pattern For Type 2 Diabetes Prevention and Treatment: Efficacy, Mechanisms, and Practical ConsiderationsDocument11 pagesPerspective: Plant-Based Eating Pattern For Type 2 Diabetes Prevention and Treatment: Efficacy, Mechanisms, and Practical ConsiderationsdgmtfmNo ratings yet
- Al., 2008. American Heart Association American Stroke AssociationDocument6 pagesAl., 2008. American Heart Association American Stroke AssociationPuput mopanggaNo ratings yet
- Natural Remedies For Heart DiseaseDocument8 pagesNatural Remedies For Heart DiseaseNur HowladerNo ratings yet
- Pathophysiology DM2, HACVDDocument2 pagesPathophysiology DM2, HACVDmitzi019No ratings yet
- FerrAurum-22: NanoSystem For Control of Symptomatic Diabetes MellitusDocument42 pagesFerrAurum-22: NanoSystem For Control of Symptomatic Diabetes MellitusdrashtiNo ratings yet
- Strokeppt 170720174010Document95 pagesStrokeppt 170720174010Venosha GunasekaranNo ratings yet
- Viva in Oral Surgery For Dental Students - Jaypee Brothers (2012) PDFDocument147 pagesViva in Oral Surgery For Dental Students - Jaypee Brothers (2012) PDFIsak Isak Isak0% (1)
- Rationale AtheroDocument6 pagesRationale AtheroMary Lorraine LoridoNo ratings yet
- 4-Key Findings From CaprieDocument30 pages4-Key Findings From CaprieMuhammad Yolandi SumadioNo ratings yet
- Jurnal HTDocument8 pagesJurnal HTseruniallisaaslimNo ratings yet
- CHFDocument35 pagesCHFNurayunie Abd HalimNo ratings yet
- Heart Disease SpeechDocument3 pagesHeart Disease Speechshamim326150% (2)
- Pharmacokinetics and PharmacodynamicsDocument166 pagesPharmacokinetics and PharmacodynamicsEvgeny BadmaevNo ratings yet
- Model Answers: Chapter 10 Transport in Humans and AnimalsDocument5 pagesModel Answers: Chapter 10 Transport in Humans and AnimalsNicole ChuaNo ratings yet
- NCP For EclampsiaDocument6 pagesNCP For EclampsiaXtine Soliman Zamora100% (3)
- (Contemporary Cardiology) Nicolas W. Shammas - Peripheral Arterial Interventions - Evolving Therapeutic Strategies-Springer (2022)Document334 pages(Contemporary Cardiology) Nicolas W. Shammas - Peripheral Arterial Interventions - Evolving Therapeutic Strategies-Springer (2022)Muhammad Azhar ImranNo ratings yet
- What Is The Function of TriglyceridesDocument5 pagesWhat Is The Function of Triglyceridesrosidin_551390No ratings yet
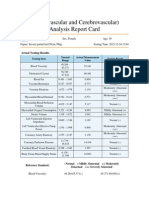
- Cardiovascular and CerebrovascularDocument6 pagesCardiovascular and CerebrovascularJoshelle B. Bancilo0% (1)
- Artemis P. Simopoulos, Francesco Visioli More On Mediterranean Diets World Review of Nutrition and Dietetics Vol 97 2006Document255 pagesArtemis P. Simopoulos, Francesco Visioli More On Mediterranean Diets World Review of Nutrition and Dietetics Vol 97 2006tazzycaNo ratings yet
- The Relationship Between Hypertension and Myocardial Infarction at Haji General Hospital Medan in 2019Document6 pagesThe Relationship Between Hypertension and Myocardial Infarction at Haji General Hospital Medan in 2019International Journal of Innovative Science and Research TechnologyNo ratings yet
- The Practice of Interventional Radiology - Valji (2012)Document753 pagesThe Practice of Interventional Radiology - Valji (2012)Nar Rungrojanarak75% (4)
- 2007 Reduction of C-Reactive Protein and The Use of Anti-HypertensivesDocument10 pages2007 Reduction of C-Reactive Protein and The Use of Anti-HypertensivesVladimir BasurtoNo ratings yet
- Fish OilsDocument36 pagesFish OilsGabiNo ratings yet
- Cholesterol Testing and The Lipid Panel - Treatment Options For Abnormal Lipid LevelsDocument6 pagesCholesterol Testing and The Lipid Panel - Treatment Options For Abnormal Lipid LevelsRatnaPrasadNalamNo ratings yet
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- Lipoprotein A Screening in Young and Middle Aged Patients Presented With Acute Vascular IschemicDocument10 pagesLipoprotein A Screening in Young and Middle Aged Patients Presented With Acute Vascular IschemicHas SimNo ratings yet
- Pathoma Lecture Notes 2017Document42 pagesPathoma Lecture Notes 2017Priyesh PrinceNo ratings yet
- HCC Training ManualDocument112 pagesHCC Training ManualKrishna Kamuni100% (1)
- Diseases of Circulatory SystemDocument40 pagesDiseases of Circulatory SystemJerrald Meyer L. BayaniNo ratings yet