You might also like
- MEATHEAD: THE SCIENCE OF GREAT BARBECUE AND GRILLING by Meathead GoldwynDocument7 pagesMEATHEAD: THE SCIENCE OF GREAT BARBECUE AND GRILLING by Meathead GoldwynHoughton Mifflin Harcourt Cookbooks67% (6)
- Pediatric NursingDocument18 pagesPediatric NursingEinjel Pearl100% (1)
- Maternal NursingDocument130 pagesMaternal NursingChristine MatasNo ratings yet
- Care of A Child With Cardiovascular DysfunctionDocument71 pagesCare of A Child With Cardiovascular DysfunctionMorgan Mitchell100% (1)
- PEDS Exam 2 - OutlineDocument67 pagesPEDS Exam 2 - OutlineBonquisha OrgamiNo ratings yet
- Maternity Nursing Lecture NotesDocument198 pagesMaternity Nursing Lecture Notesprogramgrabber75% (4)
- Pediatric NursingDocument55 pagesPediatric Nursingbajaoc100% (14)
- Peds 2301 Exam #1Document72 pagesPeds 2301 Exam #1Jenni100% (3)
- LOW RISK NEONATAL NURSING: Passbooks Study GuideFrom EverandLOW RISK NEONATAL NURSING: Passbooks Study GuideNo ratings yet
- Hersey Modern Violin MethodDocument53 pagesHersey Modern Violin Methodovidiu4u2003100% (2)
- Craft Cluster DocumentationDocument57 pagesCraft Cluster DocumentationKokila srivastava100% (3)
- The Yearling: Study GuideDocument13 pagesThe Yearling: Study GuideDaniel PalermoNo ratings yet
- Brain Teasers 2Document2 pagesBrain Teasers 2Starpiter50% (6)
- Pediatric NursingDocument102 pagesPediatric Nursingdawnmichael100% (2)
- Pediatric NursingDocument187 pagesPediatric Nursingirene8000100% (2)
- Pediatric NursingDocument46 pagesPediatric Nursingjoy de castroNo ratings yet
- Pediatric Nursing-Course AuditDocument305 pagesPediatric Nursing-Course AuditMarites Santos Aquino100% (1)
- Pediatric DiseasesDocument10 pagesPediatric DiseasesKira100% (4)
- Pediatric NursingDocument9 pagesPediatric NursingCreighton A. BayonganNo ratings yet
- Paediatric and Paediatric Nursing IDocument541 pagesPaediatric and Paediatric Nursing ILUAMFULA RHC100% (1)
- Development MCQDocument4 pagesDevelopment MCQv_vijayakanth7656No ratings yet
- Maternal Newborn NursingDocument11 pagesMaternal Newborn NursingRaf Luis100% (4)
- Growth and DevelopmentDocument44 pagesGrowth and Developmentالأغا محمد زكارنة100% (2)
- High Risk Newborn Conditions Present at BirthDocument47 pagesHigh Risk Newborn Conditions Present at BirthChinchu ChinchuNo ratings yet
- Pediatric NursingDocument37 pagesPediatric Nursingjairize100% (5)
- 1.conginital Cardiac DefectsDocument39 pages1.conginital Cardiac DefectsJõsëph Jåy MîthNo ratings yet
- Pediatric Nursing 1الجزء الأولDocument291 pagesPediatric Nursing 1الجزء الأولAhmed Elryah0% (1)
- Primary ComplexDocument24 pagesPrimary ComplexEvelyn MedinaNo ratings yet
- Growth and Development of ChildrenDocument144 pagesGrowth and Development of ChildrenHaniya KhanNo ratings yet
- High Risk NewbornDocument14 pagesHigh Risk NewbornElaisa Mae Delos Santos100% (1)
- Pediatric Nursing Edited)Document1 pagePediatric Nursing Edited)Dominique RamosNo ratings yet
- Pediatric DisorderDocument35 pagesPediatric DisorderDenaise MarieNo ratings yet
- Pediatric DisordersDocument182 pagesPediatric DisordersErnesto Trinidad Jr RN83% (6)
- Pediatric Review QUestionsDocument87 pagesPediatric Review QUestionsAnn Michelle Tarrobago89% (9)
- High Risk Newborn and FamilyDocument93 pagesHigh Risk Newborn and FamilyJen IlaganNo ratings yet
- Pediatric Nursing GuideDocument13 pagesPediatric Nursing GuideTanya Viars100% (1)
- Medical-Surgical Nursing-3Document23 pagesMedical-Surgical Nursing-3slsNo ratings yet
- Care of The NewbornDocument5 pagesCare of The Newbornbuzz Q100% (2)
- Pediatric Nursing Practice TestDocument10 pagesPediatric Nursing Practice TestEthel Gretchen Casalla71% (7)
- Maternity and Newborn Nursing ReviewerDocument40 pagesMaternity and Newborn Nursing Reviewerrahkel08No ratings yet
- Health Problems Common in PRESCHOOLDocument15 pagesHealth Problems Common in PRESCHOOLJanelle Lois EscolanoNo ratings yet
- High-Risk NewbornDocument28 pagesHigh-Risk Newborncjolou100% (2)
- PediatricDocument99 pagesPediatricGlenn Daryll Santos100% (2)
- Immediate Newborn Care-DOH 2010Document2 pagesImmediate Newborn Care-DOH 2010fegerilene100% (2)
- High-Risk Newborns and Child During Illness and Hospitalization - Pediatric NursingDocument200 pagesHigh-Risk Newborns and Child During Illness and Hospitalization - Pediatric Nursingjaggermeister20100% (8)
- Maternal NursingDocument37 pagesMaternal NursingCai Velasco DecenaNo ratings yet
- Maternal and Child LecturesDocument88 pagesMaternal and Child Lecturesjonalyn uraoNo ratings yet
- New Born Care 1Document12 pagesNew Born Care 1Tsuyoshi BangNo ratings yet
- Principles of Growth and DevelopmentDocument15 pagesPrinciples of Growth and DevelopmentAbigail MangaoangNo ratings yet
- Growth and DevelopmentDocument150 pagesGrowth and Developmentvicson_4No ratings yet
- High Risk NewbornDocument24 pagesHigh Risk NewbornYemaya84No ratings yet
- Drugs Pediatrics PDFDocument32 pagesDrugs Pediatrics PDFNaveen KovalNo ratings yet
- Medical Surgical Nursing Review NotesDocument75 pagesMedical Surgical Nursing Review NotesMary Ann Comia RañolaNo ratings yet
- Newborn ppt-1912884505Document72 pagesNewborn ppt-1912884505syahfitriA riski100% (1)
- Pediatric Q&ADocument12 pagesPediatric Q&AMateen ShukriNo ratings yet
- Chapter 032Document7 pagesChapter 032Younsholve100% (3)
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Quick Hits for Pediatric Emergency MedicineFrom EverandQuick Hits for Pediatric Emergency MedicineCristina M. Zeretzke-BienNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- The Children's Hospital of Philadelphia Guide to Asthma: How to Help Your Child Live a Healthier LifeFrom EverandThe Children's Hospital of Philadelphia Guide to Asthma: How to Help Your Child Live a Healthier LifeJulian Lewis Allen, M.D.No ratings yet
- MATERNAL AND CHILD HEALTH NURSE: Passbooks Study GuideFrom EverandMATERNAL AND CHILD HEALTH NURSE: Passbooks Study GuideNo ratings yet
- The Neurologic Examination-PDOUT-MHAMCMDocument31 pagesThe Neurologic Examination-PDOUT-MHAMCMNorjetalexis CabreraNo ratings yet
- Lonza BenchGuides Protocol For Performing A Trypan Blue Viability Test Technical Reference Guide PDFDocument2 pagesLonza BenchGuides Protocol For Performing A Trypan Blue Viability Test Technical Reference Guide PDFNorjetalexis CabreraNo ratings yet
- j.1 Emergencies 072012Document32 pagesj.1 Emergencies 072012Norjetalexis CabreraNo ratings yet
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYNorjetalexis CabreraNo ratings yet
- Drug ComputationDocument1 pageDrug ComputationNorjetalexis CabreraNo ratings yet
- 3.2 Peritoneal Cavity and The Esophagus (Banez)Document4 pages3.2 Peritoneal Cavity and The Esophagus (Banez)Norjetalexis CabreraNo ratings yet
- HodgkinDocument2 pagesHodgkinNorjetalexis CabreraNo ratings yet
- Compilation AnesthesiaDocument5 pagesCompilation AnesthesiaNorjetalexis CabreraNo ratings yet
- Etiology Demographic S Clinical Manifestation S Disease Progressio N Pathophysiolog y Microscopic Appearanc e PrognosisDocument1 pageEtiology Demographic S Clinical Manifestation S Disease Progressio N Pathophysiolog y Microscopic Appearanc e PrognosisNorjetalexis CabreraNo ratings yet
- 3.1 Anterior Abdominal Wall (Bea)Document5 pages3.1 Anterior Abdominal Wall (Bea)Norjetalexis CabreraNo ratings yet
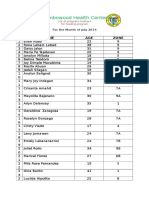
- Zambowood Health Center: Name AGE ZoneDocument2 pagesZambowood Health Center: Name AGE ZoneNorjetalexis CabreraNo ratings yet
- Drug ComputationDocument1 pageDrug ComputationNorjetalexis CabreraNo ratings yet
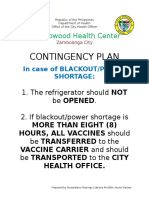
- Contingency Plan: Zambowood Health CenterDocument1 pageContingency Plan: Zambowood Health CenterNorjetalexis CabreraNo ratings yet
- Beriot Method Part 1Document78 pagesBeriot Method Part 1Norjetalexis CabreraNo ratings yet
- Parasitology Slide Presentation SET BDocument28 pagesParasitology Slide Presentation SET BNorjetalexis CabreraNo ratings yet
- Yoga and Meditation in Savasana.Document3 pagesYoga and Meditation in Savasana.yogimariNo ratings yet
- Cells and TissuesDocument14 pagesCells and TissuesLawrence NemirNo ratings yet
- Overlord - Volume 04 - The Lizardmen Heroes (Yen Press) (Ko) (Kitzoku) PDFDocument332 pagesOverlord - Volume 04 - The Lizardmen Heroes (Yen Press) (Ko) (Kitzoku) PDFAmanuealNo ratings yet
- FCE Exam 3 Reading and Use of EnglishDocument11 pagesFCE Exam 3 Reading and Use of EnglishJosué Aguilar PalominoNo ratings yet
- FCE Test SampleDocument5 pagesFCE Test SamplelennihollanderNo ratings yet
- Reindeer BookletDocument16 pagesReindeer BookletAlejandra HernándezNo ratings yet
- All On 4 ConceptDocument5 pagesAll On 4 ConceptaakankshakanwarNo ratings yet
- RADA in Business - Effective Communication ManualDocument37 pagesRADA in Business - Effective Communication ManualGabriel Mendoza VargasNo ratings yet
- The Laws Detailed in The Book of LeviticusDocument14 pagesThe Laws Detailed in The Book of Leviticusdanceswithwinkles100% (3)
- Bull Race in Ramgarh - Ludhiana: OIPA in India Lodged Complaint For Legal Action and Rescue of Abused Animals - Naresh KadyanDocument4 pagesBull Race in Ramgarh - Ludhiana: OIPA in India Lodged Complaint For Legal Action and Rescue of Abused Animals - Naresh KadyanNaresh KadyanNo ratings yet
- Egg Cookery PowerpointDocument43 pagesEgg Cookery PowerpointBossy Thing'sNo ratings yet
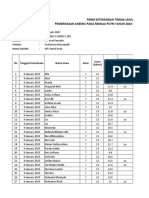
- Pemeriksaan Anemia SMP Darul MaarifDocument38 pagesPemeriksaan Anemia SMP Darul MaarifPuskesmas BanyuputihNo ratings yet
- Environmental Law: Submitted By: Submitted To: Jan Vernon L. Hernan Ambassador Tolentino 2ADocument6 pagesEnvironmental Law: Submitted By: Submitted To: Jan Vernon L. Hernan Ambassador Tolentino 2AJavi HernanNo ratings yet
- Introducing The DogDocument22 pagesIntroducing The DogPope SmithNo ratings yet
- Diabetes Mellitus (DM) 2Document1 pageDiabetes Mellitus (DM) 2Bheru Lal100% (1)
- 34 English Spelling TodayDocument13 pages34 English Spelling TodayabdulmusaverNo ratings yet
- Jackson County Fair Preview 072811Document6 pagesJackson County Fair Preview 072811Livewire Printing CompanyNo ratings yet
- Uh Bahasa Inggris (Preposition of Place)Document3 pagesUh Bahasa Inggris (Preposition of Place)nailu hanun al haq90% (10)
- 3 - Meiosis Notes - WeeblyDocument42 pages3 - Meiosis Notes - Weeblyapi-375285021No ratings yet
- FeygodsDocument6 pagesFeygodsZhori DuberryNo ratings yet
- Skills Test Unit 2 Test ADocument6 pagesSkills Test Unit 2 Test ANastyusha Shapoval50% (2)
- 1.andersen: 2. BimlerDocument6 pages1.andersen: 2. BimlerRoxana ElenaNo ratings yet
- De Waal, F. 2014. The Bonobo and The Atheist. in Search of Humanism Among The Primates PDFDocument4 pagesDe Waal, F. 2014. The Bonobo and The Atheist. in Search of Humanism Among The Primates PDFMelchiorNo ratings yet
- Chinese Metasoft: Home Products Da Liu Ren Ba Zi Qi Men Dun Jia Feng Shui Ze RiDocument1 pageChinese Metasoft: Home Products Da Liu Ren Ba Zi Qi Men Dun Jia Feng Shui Ze RiFingiel BluNo ratings yet
- Coronary Artery Disease - Case StudyDocument19 pagesCoronary Artery Disease - Case StudyJulieteeySarania100% (3)
- Ket CambridgeDocument23 pagesKet Cambridgeo100No ratings yet