You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Lecture 30 - Pathology of AtherosclerosisDocument43 pagesLecture 30 - Pathology of Atherosclerosisapi-3703352100% (6)
- 1-2 Hemostasis PhysiologyDocument48 pages1-2 Hemostasis PhysiologyHussein Al Saedi100% (2)
- 5 DISEASES OF THE CARDIOVASCULAR SYSTEMDocument24 pages5 DISEASES OF THE CARDIOVASCULAR SYSTEMHussein Al SaediNo ratings yet
- 5 DISEASES OF THE CARDIOVASCULAR SYSTEMDocument24 pages5 DISEASES OF THE CARDIOVASCULAR SYSTEMHussein Al SaediNo ratings yet
- Vascular Diseases - CJ.Document12 pagesVascular Diseases - CJ.Catherine Jung100% (1)
- Bailey and Love Surgery Mcqs PDFDocument10 pagesBailey and Love Surgery Mcqs PDFHussein Al Saedi78% (9)
- Emergency in Vascular SurgeryDocument74 pagesEmergency in Vascular Surgerysteven andreanNo ratings yet
- Carbohydrate MetabolismDocument38 pagesCarbohydrate Metabolismwidya nurrohmanNo ratings yet
- Radiology SpottersDocument58 pagesRadiology SpottersPartha Ganesan33% (3)
- Diseases of The Cvs AnswersDocument21 pagesDiseases of The Cvs AnswersHussein Al SaediNo ratings yet
- Bone and Joint Disease: Involve The Vertebrae Pott DiseaseDocument5 pagesBone and Joint Disease: Involve The Vertebrae Pott DiseaseHussein Al SaediNo ratings yet
- HistoryDocument10 pagesHistoryHussein Al SaediNo ratings yet
- Urinary Tract InfectionDocument30 pagesUrinary Tract InfectionHussein Al SaediNo ratings yet
- Blood Physiology: Resistance of The Body To Infection: Immunity and AllergyDocument25 pagesBlood Physiology: Resistance of The Body To Infection: Immunity and AllergyHussein Al Saedi100% (1)
- Paediatric SurgeryDocument2 pagesPaediatric SurgeryHussein Al SaediNo ratings yet
- Formula FeedingDocument13 pagesFormula FeedingHussein Al SaediNo ratings yet
- Fracture Neck FemurDocument34 pagesFracture Neck FemurHussein Al SaediNo ratings yet
- Ischemic Heart DiseaseDocument7 pagesIschemic Heart DiseaseHussein Al SaediNo ratings yet
- Minerial, 2ed Class, BiochemistryDocument29 pagesMinerial, 2ed Class, BiochemistryHussein Al SaediNo ratings yet
- Giardiasis 2013-2014Document72 pagesGiardiasis 2013-2014Hussein Al SaediNo ratings yet
- Recommendation for Iraqi Exchange ProgramDocument2 pagesRecommendation for Iraqi Exchange ProgramHussein Al SaediNo ratings yet
- 025b MetabolismDocument35 pages025b MetabolismCosminaaaaaaaaNo ratings yet
- 2014 I y Lep Student RecommendationDocument4 pages2014 I y Lep Student RecommendationHussein Al SaediNo ratings yet
- Hemodynamic DisordersDocument16 pagesHemodynamic DisordersHussein Al SaediNo ratings yet
- PELVISDocument9 pagesPELVISHussein Al SaediNo ratings yet
- ABDOMENDocument16 pagesABDOMENHussein Al SaediNo ratings yet
- Carb OverviewDocument30 pagesCarb OverviewHussein Al SaediNo ratings yet
- IIDocument10 pagesIIHussein Al SaediNo ratings yet
- The Skull PDFDocument42 pagesThe Skull PDFHussein Al SaediNo ratings yet
- L 1cholinergics & AnticholinergicsDocument18 pagesL 1cholinergics & AnticholinergicsHussein Al SaediNo ratings yet
- Carbohydrate MetabolismDocument30 pagesCarbohydrate MetabolismJayvee C. DizonNo ratings yet
- Metabolism Exam Questions2Document4 pagesMetabolism Exam Questions2Hussein Al SaediNo ratings yet
- NNDocument7 pagesNNHussein Al SaediNo ratings yet
- Potter, Perry, (2010) - Fundamental of Nursing Fundamental Keperawatan, Ed 7 Buku 2Document3 pagesPotter, Perry, (2010) - Fundamental of Nursing Fundamental Keperawatan, Ed 7 Buku 2KelvinNo ratings yet
- Arterial Thrombosis by AbrarDocument20 pagesArterial Thrombosis by AbrarZain HadiNo ratings yet
- 33 Penyakit Vaskuler Sentral Dan Perifer DR - WinangunDocument69 pages33 Penyakit Vaskuler Sentral Dan Perifer DR - WinangunSurya ArhNo ratings yet
- Dr. Rahmah Safitri Meutia's Career History and Hypertension GuideDocument39 pagesDr. Rahmah Safitri Meutia's Career History and Hypertension GuidedhestiNo ratings yet
- Angina PectorisDocument3 pagesAngina PectorisGwyn Oona Florence ForroNo ratings yet
- Template For HPN and DM MasterlistDocument12 pagesTemplate For HPN and DM MasterlistJoelChris LicayanNo ratings yet
- TutorialDocument18 pagesTutorialEllya Syahfitri 2108125983No ratings yet
- AtherosclerosisDocument5 pagesAtherosclerosisJoanne LagusadNo ratings yet
- Pathophysiology of StrokeDocument20 pagesPathophysiology of StrokeDeaNo ratings yet
- Stroke Hemoragik (DR - Dr. Syahrul, SPS (K) )Document25 pagesStroke Hemoragik (DR - Dr. Syahrul, SPS (K) )YogaNo ratings yet
- Predisposing and precipitating factors of abdominal aortic aneurysmDocument6 pagesPredisposing and precipitating factors of abdominal aortic aneurysmSandrine BarredoNo ratings yet
- Acute Coronary Syndrome Update: Charles Shoalmire, MSN, RN, ACNP-BCDocument31 pagesAcute Coronary Syndrome Update: Charles Shoalmire, MSN, RN, ACNP-BCDwi Akbarina YahyaNo ratings yet
- FriS41700 PhlegmasiaCeruleaDolensisaLimbThreateningProblem BhendeDocument54 pagesFriS41700 PhlegmasiaCeruleaDolensisaLimbThreateningProblem BhendeSuren VishvanathNo ratings yet
- Blood Clot in The BrainDocument3 pagesBlood Clot in The BrainHarsh KananiNo ratings yet
- Amniotic Fluid EmbolismDocument27 pagesAmniotic Fluid EmbolismDavichín LCNo ratings yet
- Monitoring Hipertensi Andi NasirDocument6 pagesMonitoring Hipertensi Andi NasirBabay JamNo ratings yet
- Dorset County Hospital NHS Foundation TrustDocument1 pageDorset County Hospital NHS Foundation TrustRika FitriaNo ratings yet
- Disorders affecting blood flow in peripheral arteries and veinsDocument2 pagesDisorders affecting blood flow in peripheral arteries and veinsrasheedNo ratings yet
- Antianginal Agents - PharmacologyDocument3 pagesAntianginal Agents - PharmacologyChona FontanillaNo ratings yet
- Ischemic Heart DiseaseDocument4 pagesIschemic Heart DiseaseBanana CakeNo ratings yet
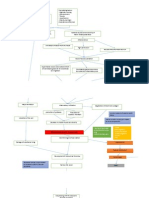
- Concept Map Joshua ValdrizDocument1 pageConcept Map Joshua ValdrizJoshua ValdrizNo ratings yet
- Cerebrovascular AccidentDocument12 pagesCerebrovascular AccidentMarvie JOiz AnteNo ratings yet
- Ait Nejm 2020Document9 pagesAit Nejm 2020Ahmed JallouliNo ratings yet
- Tentorial Subdural Hematoma Following Hypertension - A Case StudyDocument3 pagesTentorial Subdural Hematoma Following Hypertension - A Case StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Update Penatalaksanaan StrokeDocument57 pagesUpdate Penatalaksanaan Strokemaryanti HennyNo ratings yet
- Li 2012Document6 pagesLi 2012Spica RegulusNo ratings yet