You might also like
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- BlsDocument9 pagesBlsGhia Iane Galicia SalvaNo ratings yet
- First Aid Essentials for Life Saving (39Document64 pagesFirst Aid Essentials for Life Saving (39KBDNo ratings yet
- CPR ALS ProcedureDocument10 pagesCPR ALS ProcedureTanmoyNo ratings yet
- Basic Life Support For Adult: Evaluating ResponsivenessDocument4 pagesBasic Life Support For Adult: Evaluating ResponsivenessJulang FahmanNo ratings yet
- BLS - BSN 2023Document90 pagesBLS - BSN 2023kenyaga JobNo ratings yet
- CPR Guide for Adults, Children & BabiesDocument6 pagesCPR Guide for Adults, Children & Babiesrupali gahalian100% (2)
- BLS Guide: Adult Basic Life Support StepsDocument50 pagesBLS Guide: Adult Basic Life Support StepsVijay Krishna Murthy80% (5)
- Adult Basic Life Support: Resuscitation Council (UK)Document14 pagesAdult Basic Life Support: Resuscitation Council (UK)Agus PriyantoNo ratings yet
- Basic LifeDocument33 pagesBasic LifetmschppmNo ratings yet
- First Aid Prenciples E-VerDocument54 pagesFirst Aid Prenciples E-Verapi-205902640100% (1)
- BLS Skills Lab For SimulationDocument116 pagesBLS Skills Lab For Simulationczeremar chan100% (1)
- Mod 3.1 - 4.1 - First AidDocument72 pagesMod 3.1 - 4.1 - First Aidabhishek sudheerNo ratings yet
- What Is Cardiac Arrest?: How Is CPR Performed?Document3 pagesWhat Is Cardiac Arrest?: How Is CPR Performed?Andrew PetalloNo ratings yet
- Lab 1: Basic Life SupportDocument16 pagesLab 1: Basic Life Supportj.doe.hex_87No ratings yet
- BLS AlgorithmDocument9 pagesBLS AlgorithmDr VJ GeorgeNo ratings yet
- Basic Life Support: Submitted By: Kennedy V. Velasco Bscrim 1-AlphaDocument7 pagesBasic Life Support: Submitted By: Kennedy V. Velasco Bscrim 1-AlphaProsperJuan BelieversNo ratings yet
- Chapter 5 EMERGENCY TREATMENTDocument22 pagesChapter 5 EMERGENCY TREATMENTEmmaNo ratings yet
- BLS Basics: Scene Safety, Circulation, Airway, BreathingDocument118 pagesBLS Basics: Scene Safety, Circulation, Airway, Breathingharpreet100% (1)
- Bls - Fbao - First AidDocument172 pagesBls - Fbao - First AidMaria Regina Castro Gabriel100% (1)
- Pediatric Basic Life Support: Philippine Heart Association Council On Cardio-Pulmonary ResuscitationDocument106 pagesPediatric Basic Life Support: Philippine Heart Association Council On Cardio-Pulmonary Resuscitationjitendra magarNo ratings yet
- Bls Question 1Document7 pagesBls Question 1balderas135384No ratings yet
- Basic Life SupportDocument4 pagesBasic Life Supportraven_claw25No ratings yet
- Adult BLS SequenceDocument2 pagesAdult BLS Sequencerikirdn27No ratings yet
- Masuri Prim AjutorDocument143 pagesMasuri Prim AjutorHojbota Otilia Constantina100% (1)
- CPR 1Document12 pagesCPR 1Renju JoseNo ratings yet
- CPR Program Objectives and TechniquesDocument7 pagesCPR Program Objectives and TechniquesragsyragsyNo ratings yet
- Basic Life Support HandoutDocument13 pagesBasic Life Support HandoutmdavaoNo ratings yet
- Cardiopulmonary Resuscitation: Mrs. Jenitta. G Lecturer/Asst - ProfessorDocument17 pagesCardiopulmonary Resuscitation: Mrs. Jenitta. G Lecturer/Asst - ProfessorCheran Devi100% (1)
- How To CPRDocument4 pagesHow To CPRRosi ArristaNo ratings yet
- Adult BLSDocument50 pagesAdult BLSdianNo ratings yet
- Lesson 4 A Basic Life SupportDocument49 pagesLesson 4 A Basic Life SupportJames Artajo ViajedorNo ratings yet
- Mod12 EmergencyFirst AidDocument29 pagesMod12 EmergencyFirst AidMhanna AYNo ratings yet
- Essentials of CPR: Lifesaving Steps for Cardiac EmergenciesDocument8 pagesEssentials of CPR: Lifesaving Steps for Cardiac Emergencieshiba majidNo ratings yet
- ACLSDocument78 pagesACLSKajalNo ratings yet
- BLS Algorithms and Training 2020Document22 pagesBLS Algorithms and Training 2020Ronald Aranha100% (1)
- BLS Healthcare ProvidersDocument8 pagesBLS Healthcare ProviderscmurphNo ratings yet
- LA Union: PDRRM ODocument32 pagesLA Union: PDRRM OEnash RidNo ratings yet
- 3.1 Introduction To First Aid and CPRDocument5 pages3.1 Introduction To First Aid and CPRPriyanshu BalaniNo ratings yet
- BASIC LIFE SUPPORT CPRDocument28 pagesBASIC LIFE SUPPORT CPRaefgNo ratings yet
- Cardiopulmonary Resuscitation (CPR)Document18 pagesCardiopulmonary Resuscitation (CPR)Althea Amor CambarijanNo ratings yet
- CPR For AdultsDocument1 pageCPR For Adultsevelyn kNo ratings yet
- BLS FinalDocument47 pagesBLS Finalshouvik chowdhury100% (1)
- BLS and First Aid ReportDocument4 pagesBLS and First Aid ReportAriane Joyce AgkisNo ratings yet
- How To Do CPR On An AdultDocument25 pagesHow To Do CPR On An AdultabNo ratings yet
- C.P.R. (1)Document19 pagesC.P.R. (1)sxm2901No ratings yet
- Basic Life SupportDocument36 pagesBasic Life SupportycccaNo ratings yet
- First Aid Is An Immediate and Temporary Care Given Mapeh Lesson 3 3rd QuarterDocument3 pagesFirst Aid Is An Immediate and Temporary Care Given Mapeh Lesson 3 3rd QuarterJanix MagbanuaNo ratings yet
- How To Perform CPRDocument2 pagesHow To Perform CPRAmirul AzhanNo ratings yet
- Cardio-Pulmonary Resuscitation (CPR)Document18 pagesCardio-Pulmonary Resuscitation (CPR)Savita HanamsagarNo ratings yet
- BLS Study Guide PDFDocument12 pagesBLS Study Guide PDFPingChavez100% (1)
- Ace Personal Trainer Manual Chapter 16Document18 pagesAce Personal Trainer Manual Chapter 16Đạt NguyễnNo ratings yet
- Cardiopulmonary ResuscitationDocument38 pagesCardiopulmonary ResuscitationAgus SyaifudinNo ratings yet
- CPR PresentationDocument22 pagesCPR PresentationAlan HabalNo ratings yet
- BLS PresentationDocument36 pagesBLS PresentationRishabh MittalNo ratings yet
- BLS & AclsDocument112 pagesBLS & AclsPriya SharmaNo ratings yet
- Untrained. If You're Not Trained in CPR, Then Provide Hands-Only CPR. ThatDocument12 pagesUntrained. If You're Not Trained in CPR, Then Provide Hands-Only CPR. ThatClaire DayritNo ratings yet
- PALS Overview for BLS and Healthcare ProvidersDocument26 pagesPALS Overview for BLS and Healthcare Providersmonir61No ratings yet
- BLS Algorithms and Training 2019: (Basic Life Support)Document21 pagesBLS Algorithms and Training 2019: (Basic Life Support)Haidir MuhammadNo ratings yet
- SepsisDocument285 pagesSepsismirzaoctaNo ratings yet
- ACLS AlgorithmsDocument14 pagesACLS AlgorithmsArif KurniadiNo ratings yet
- Drip ChartDocument10 pagesDrip Chartmirzaocta100% (1)
- Panduan Pelayanan BedahDocument3 pagesPanduan Pelayanan BedahAndris PurwaningtiasNo ratings yet
- Buku AnestesiDocument33 pagesBuku AnestesiAan AnharNo ratings yet
- Thyroid Disease Anesthetic ConsiderationsDocument30 pagesThyroid Disease Anesthetic ConsiderationsmirzaoctaNo ratings yet
- Systemic Response To InjuryDocument20 pagesSystemic Response To InjurymirzaoctaNo ratings yet
- Hand Washing PDFDocument1 pageHand Washing PDFmirzaoctaNo ratings yet
- 5momentsHandHygiene A3 PDFDocument1 page5momentsHandHygiene A3 PDFDwi SurantoNo ratings yet
- Bls 2013Document12 pagesBls 2013mirzaocta100% (1)
- CV TITLEDocument3 pagesCV TITLEAdraNo ratings yet
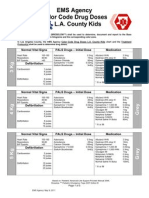
- EMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationDocument5 pagesEMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationCruz VerdeNo ratings yet
- Airway and The NurseDocument7 pagesAirway and The NursecarmenbuleandraNo ratings yet
- Phecc CPG 2021 - Far Web3Document69 pagesPhecc CPG 2021 - Far Web3James McloughlinNo ratings yet
- Advance Life SupportDocument198 pagesAdvance Life SupportPantelis PouliopoulosNo ratings yet
- A Systematic Approach To EMS Cardiac Arrest Management Improves Survival For Out of Hospital Cardiac ArrestDocument29 pagesA Systematic Approach To EMS Cardiac Arrest Management Improves Survival For Out of Hospital Cardiac ArrestMELLYNDA ANASTASYANo ratings yet
- Ground Ambulance Services in The United States - A FAIR Health White PaperDocument31 pagesGround Ambulance Services in The United States - A FAIR Health White PaperepraetorianNo ratings yet
- Medical Plan ICS 206Document2 pagesMedical Plan ICS 206Alo RioNo ratings yet
- Advanced Life Support Algorithm: Version: July 2016Document45 pagesAdvanced Life Support Algorithm: Version: July 2016Dwi RinaNo ratings yet
- Cardio Pulmonary ResuscitationDocument8 pagesCardio Pulmonary ResuscitationRuchika Kaushal71% (7)
- BLS and ACLS GuidelinesDocument46 pagesBLS and ACLS GuidelinesmirzaoctaNo ratings yet
- Aea-V 2009 EbaDocument110 pagesAea-V 2009 EbaDave JonesNo ratings yet
- Advanced Life Support Training and Assessment PDFDocument6 pagesAdvanced Life Support Training and Assessment PDFwilmaNo ratings yet
- EMS Alphabet SoupDocument3 pagesEMS Alphabet SoupCourtney0% (1)
- Agreement AmbulanceDocument3 pagesAgreement AmbulanceVIKAS PANERI100% (2)
- Emergency Medical Services Pre-Hospital Treatment Protocols: Complete Text Eighth Edition Effective 3/1/2010Document257 pagesEmergency Medical Services Pre-Hospital Treatment Protocols: Complete Text Eighth Edition Effective 3/1/2010Slaviša KovačevićNo ratings yet
- 2.1 Algoritmos AHA 2020Document22 pages2.1 Algoritmos AHA 2020Lorena Angarita RamirezNo ratings yet
- Convention Centre Detailed InfoDocument43 pagesConvention Centre Detailed InfoSaranya Saru100% (1)
- Basic Life Support and Advanced Cardiac Life Support: Knowledge of Medical Students in New DelhiDocument9 pagesBasic Life Support and Advanced Cardiac Life Support: Knowledge of Medical Students in New DelhiSriatiNo ratings yet
- Warren More Emergency Medical Services Personnel and Increased Survival After OHCADocument9 pagesWarren More Emergency Medical Services Personnel and Increased Survival After OHCAJamison ParfittNo ratings yet
- Manipal Manual of Resuscitation - 4th EditionDocument73 pagesManipal Manual of Resuscitation - 4th EditionAshlita Mendonca100% (2)
- ALS AlgorithmDocument22 pagesALS AlgorithmBookwormNo ratings yet
- Advanced Life Support Protocol Update 2006Document59 pagesAdvanced Life Support Protocol Update 2006Dennis Nabor Muñoz, RN,RM100% (3)
- Advanced Life Support-RESSU CouncilDocument30 pagesAdvanced Life Support-RESSU CouncilGigel DumitruNo ratings yet
- 25 E.D Questions With RationaleDocument12 pages25 E.D Questions With RationaleRhose Angel AzurNo ratings yet
- 3 (NCORT) Guidelines For Resuscitation Training in Ministry of Health Malaysia Hospitals & Healthcare Facilities PDFDocument66 pages3 (NCORT) Guidelines For Resuscitation Training in Ministry of Health Malaysia Hospitals & Healthcare Facilities PDFDzarrinNo ratings yet
- Charleston County Clinical Operating Guidelines: Adult & PediatricDocument207 pagesCharleston County Clinical Operating Guidelines: Adult & PediatricJohn DodsonNo ratings yet
- Erc - Sva 2021Document37 pagesErc - Sva 2021Vinícius MenegatNo ratings yet
- NZRC - All Adult Advanced Life Support Guidelines3Document79 pagesNZRC - All Adult Advanced Life Support Guidelines3stanwalksNo ratings yet