You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Thumb Spica Cast 1Document1 pageThumb Spica Cast 1lxnalexanderNo ratings yet
- Sti Health Topic For JulyDocument35 pagesSti Health Topic For JulylxnalexanderNo ratings yet
- BREAST Ca 2Document3 pagesBREAST Ca 2lxnalexanderNo ratings yet
- BPHDocument4 pagesBPHlxnalexanderNo ratings yet
- Asuogyaman TB 2009Document19 pagesAsuogyaman TB 2009lxnalexanderNo ratings yet
- ENT Lectures 1Document123 pagesENT Lectures 1lxnalexander100% (1)
- Thyroid HXDocument3 pagesThyroid HXlxnalexanderNo ratings yet
- Pregnancy Loss AbortionsDocument5 pagesPregnancy Loss AbortionslxnalexanderNo ratings yet
- The Chps ConceptDocument16 pagesThe Chps Conceptlxnalexander100% (1)
- Gastric Outlet Obstruction: AgonaDocument4 pagesGastric Outlet Obstruction: AgonalxnalexanderNo ratings yet
- Incisional HerniaDocument3 pagesIncisional HernialxnalexanderNo ratings yet
- Thyroid HXDocument3 pagesThyroid HXlxnalexanderNo ratings yet
- QUIZ II PolyneuropathyDocument7 pagesQUIZ II PolyneuropathylxnalexanderNo ratings yet
- ENT Lectures 1Document123 pagesENT Lectures 1lxnalexander100% (1)
- Neonatal Surg - EmergDocument23 pagesNeonatal Surg - EmerglxnalexanderNo ratings yet
- Quiz V DkaDocument8 pagesQuiz V DkalxnalexanderNo ratings yet
- Carcinoma of The ProstateDocument32 pagesCarcinoma of The ProstatelxnalexanderNo ratings yet
- Group Test Cord CompressionDocument7 pagesGroup Test Cord CompressionlxnalexanderNo ratings yet
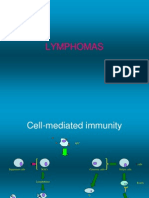
- LymphomasDocument22 pagesLymphomaslxnalexanderNo ratings yet
- HIV Disease Clinical Vignettes and CasesDocument26 pagesHIV Disease Clinical Vignettes and CaseslxnalexanderNo ratings yet
- Patient in Shock: DR I. K. OwusuDocument26 pagesPatient in Shock: DR I. K. OwusulxnalexanderNo ratings yet
- Anaemia IDocument22 pagesAnaemia IlxnalexanderNo ratings yet
- The Mental State ExaminationDocument14 pagesThe Mental State ExaminationlxnalexanderNo ratings yet
- Patient With Jaundice and AscitesDocument31 pagesPatient With Jaundice and AsciteslxnalexanderNo ratings yet
- Psychiatry and Organic CausesDocument22 pagesPsychiatry and Organic CauseslxnalexanderNo ratings yet
- Davidson's McqsDocument145 pagesDavidson's McqsSekhons Akademy100% (3)
- Clinical Examination of A Diabetic Patient ErDocument38 pagesClinical Examination of A Diabetic Patient Erlxnalexander100% (1)
- Psychiatric EmergenciesDocument7 pagesPsychiatric EmergencieslxnalexanderNo ratings yet
- Effects of Alcohol and Substance MisuseDocument8 pagesEffects of Alcohol and Substance MisuselxnalexanderNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Baterial & Fungal Corneal UlcersDocument28 pagesBaterial & Fungal Corneal UlcersVasishta NadellaNo ratings yet
- Biology Curriculum MapDocument2 pagesBiology Curriculum Mapapi-644434957No ratings yet
- Nur 097 Sas 1 3Document9 pagesNur 097 Sas 1 3gekkonoojiNo ratings yet
- Biochemistry Assignment: On Acid-Base BalanceDocument4 pagesBiochemistry Assignment: On Acid-Base BalanceMuhammed ElRakabawiNo ratings yet
- Project Report For 9000Document10 pagesProject Report For 9000GOLLAVILLI GANESH100% (1)
- Definition of Anatomy and PhysiologyDocument2 pagesDefinition of Anatomy and Physiologybradia_03686330No ratings yet
- Medicine in Allen: Sensitive TouchDocument38 pagesMedicine in Allen: Sensitive TouchAyeshik ChakrabortyNo ratings yet
- CRH Radiology Policies and ProceduresDocument60 pagesCRH Radiology Policies and ProceduresAbdul Saeed Shah100% (1)
- Indian Herbs Cooking GuideDocument37 pagesIndian Herbs Cooking Guidehitesh mendirattaNo ratings yet
- Atc DDD OlukaDocument65 pagesAtc DDD Olukarini setyawatiNo ratings yet
- To Remember The Four Causes of Cell InjuryDocument43 pagesTo Remember The Four Causes of Cell Injuryapi-3825096No ratings yet
- Comparison and Summary of Types of ArthritisDocument2 pagesComparison and Summary of Types of ArthritisShaz Chindhy50% (2)
- A 55-Year-Old Woman With Shock and Labile Blood PressureDocument11 pagesA 55-Year-Old Woman With Shock and Labile Blood PressureMr. LNo ratings yet
- F7.6 Seafarers Medical Examination-CertificateDocument7 pagesF7.6 Seafarers Medical Examination-CertificateHerbert Maganga100% (1)
- BL42-Chi Nei Tsang III (ID-PDF) 12-17-15 PDFDocument90 pagesBL42-Chi Nei Tsang III (ID-PDF) 12-17-15 PDFJosé Tao75% (8)
- Epstein Barr VirusDocument13 pagesEpstein Barr VirusDianaLorenaNo ratings yet
- MNT For Sucrase Isomaltase DeficiencyDocument14 pagesMNT For Sucrase Isomaltase DeficiencySarah DresselNo ratings yet
- Alex Cox Death 911 Call TranscriptDocument10 pagesAlex Cox Death 911 Call Transcripttmiller696733% (3)
- The Neurological History Taking: Osheik Seidi Sunderland Royal Hospital UKDocument38 pagesThe Neurological History Taking: Osheik Seidi Sunderland Royal Hospital UKHassen Kavi Isse100% (3)
- KRF Guideline Chest KeloidsDocument29 pagesKRF Guideline Chest Keloidscanciondemayo3358No ratings yet
- Parasitology study table overviewDocument10 pagesParasitology study table overviewBashaer GellehNo ratings yet
- Congenital SyphilisDocument28 pagesCongenital SyphilisMeena Koushal100% (4)
- AcupunctureDocument15 pagesAcupuncturezextorcNo ratings yet
- Pug BookDocument152 pagesPug BookArtemio SotomayorNo ratings yet
- EGurukul GlaucomaDocument15 pagesEGurukul GlaucomaOscar Daniel Mendez100% (1)
- Superannuation Benefits SessionDocument49 pagesSuperannuation Benefits SessionfunshareNo ratings yet
- CPT ComprehensiveDocument14 pagesCPT Comprehensivesha100% (1)
- Kelas 3Document5 pagesKelas 3RojNo ratings yet
- Nephrotic Syndrome - NotesDocument22 pagesNephrotic Syndrome - NotesHampson Malekano100% (1)
- FundaDocument5 pagesFundaGreggy Francisco LaraNo ratings yet