You might also like
- El-Chaar - Introduction To Pediatric PharmacotherapyDocument85 pagesEl-Chaar - Introduction To Pediatric PharmacotherapyTaj PolinNo ratings yet
- Giving Children Medicines SafelyDocument36 pagesGiving Children Medicines SafelyJonathanNo ratings yet
- Drugs in Pediatric Pts NURS 310 Pinson Wi - 16Document42 pagesDrugs in Pediatric Pts NURS 310 Pinson Wi - 16Abdiweli AbubakarNo ratings yet
- Pediatric MedicationsDocument27 pagesPediatric MedicationsKzie Rivera100% (1)
- General Prescribing Guidelines of Pedriatic PatientsDocument11 pagesGeneral Prescribing Guidelines of Pedriatic PatientsGloomi100% (1)
- Kesehatan Anak 111219b DR Isnatin Merec Bulletin Vol11 No2Document4 pagesKesehatan Anak 111219b DR Isnatin Merec Bulletin Vol11 No2Gianina Yogy100% (1)
- Medicine Policy 2011Document10 pagesMedicine Policy 2011centralwebadminNo ratings yet
- Pharmacology A Patient Centered Nursing Process Approach Kee 8th Edition Test Bank Full DownloadDocument7 pagesPharmacology A Patient Centered Nursing Process Approach Kee 8th Edition Test Bank Full Downloadchristinehallpkadrcnjxs100% (42)
- NUTRIONDocument11 pagesNUTRIONZuhaib AhmedNo ratings yet
- Lehnes Pharmacology For Nursing Care 10th Edition Burchum Test BankDocument5 pagesLehnes Pharmacology For Nursing Care 10th Edition Burchum Test Bankbrandoncoletjaxprigfm100% (28)
- 24 0 PDFDocument12 pages24 0 PDFAna-Mihaela BalanutaNo ratings yet
- Common Paediatric Concerns, Complications During Drug TherapyDocument16 pagesCommon Paediatric Concerns, Complications During Drug TherapyRubinaNo ratings yet
- Drug Therapy Across The LifespanDocument34 pagesDrug Therapy Across The LifespanJSeasharkNo ratings yet
- 565-Article Text-2680-1-10-20230702Document7 pages565-Article Text-2680-1-10-20230702Yosep SembiringNo ratings yet
- B. Intro To PharmaDocument18 pagesB. Intro To PharmaJedelyn GarciaNo ratings yet
- CPT 2nd ChapDocument33 pagesCPT 2nd ChapTarun GuruvelliNo ratings yet
- Drug Therapy in Neonates & InfantsDocument19 pagesDrug Therapy in Neonates & InfantsPearlNo ratings yet
- Drug Therapy During Pregnancy and Breast-FeedingDocument52 pagesDrug Therapy During Pregnancy and Breast-FeedingSonam SonamNo ratings yet
- NURSING PROCESS in DRUG THERAPYDocument4 pagesNURSING PROCESS in DRUG THERAPYMichiko CiriacoNo ratings yet
- SyllabusDocument7 pagesSyllabusMagesh MagiNo ratings yet
- Building a Healthy Child: Food Introduction Nutritional Program—A Parent’S Guide to Foundational Childhood Nutrition for Lifelong HealthFrom EverandBuilding a Healthy Child: Food Introduction Nutritional Program—A Parent’S Guide to Foundational Childhood Nutrition for Lifelong HealthNo ratings yet
- Breastfeeding & Psychiatric Medications - MGH Centerfor Women's Mental Health (2022)Document7 pagesBreastfeeding & Psychiatric Medications - MGH Centerfor Women's Mental Health (2022)José Antonio Alves VilelaNo ratings yet
- Medication Administration Guide for NursesDocument4 pagesMedication Administration Guide for Nursesmysoftware01No ratings yet
- C. Pharmacology in NursingDocument34 pagesC. Pharmacology in NursingTricia Mae BayubayNo ratings yet
- Session #16 SAS - Nutrition (Lecture)Document6 pagesSession #16 SAS - Nutrition (Lecture)cabo.bontilao.swuNo ratings yet
- Contemporary IssuesDocument47 pagesContemporary IssuesAnnette Aquino GuevarraNo ratings yet
- PosologyDocument24 pagesPosologyBhavin PandyaNo ratings yet
- Pos OlogyDocument25 pagesPos OlogyMonica MuruganNo ratings yet
- Obesity General Presentation: Body Mass Index (BMI) Is Calculated As Weight (KG) Divided by Height Squared (MDocument8 pagesObesity General Presentation: Body Mass Index (BMI) Is Calculated As Weight (KG) Divided by Height Squared (MAssma Haytham MuradNo ratings yet
- Oral Medication AdministrationDocument11 pagesOral Medication AdministrationMayank KumarNo ratings yet
- Farmakoterapi Pada Kelompok Khusus: Fathiyah Safithri Laboratorium Farmakologi FK-UMM 2009Document60 pagesFarmakoterapi Pada Kelompok Khusus: Fathiyah Safithri Laboratorium Farmakologi FK-UMM 2009Yasmin AlqadriNo ratings yet
- Farmakoterapi Kelompok Khusus dan Ibu HamilDocument60 pagesFarmakoterapi Kelompok Khusus dan Ibu HamilYasmin AlqadriNo ratings yet
- Medication Use in Older Adults by Rose Knapp, MSN, RN, APRN-BC, ANPDocument34 pagesMedication Use in Older Adults by Rose Knapp, MSN, RN, APRN-BC, ANPJose Antonio Tous OlagortaNo ratings yet
- Calculating Pediatric and Geriatric Drug Doses Based on Patient ParametersDocument7 pagesCalculating Pediatric and Geriatric Drug Doses Based on Patient ParametersRyan Charles Uminga GalizaNo ratings yet
- Pediatric Drug Calculations 03Document38 pagesPediatric Drug Calculations 03Leia Avriele TankiamcoNo ratings yet
- Hospital Formulary: Astralis Medical GroupDocument36 pagesHospital Formulary: Astralis Medical GroupJade MBNo ratings yet
- Digestive Wellness for Children: How to Stengthen the Immune System & Prevent Disease Through Healthy DigestionFrom EverandDigestive Wellness for Children: How to Stengthen the Immune System & Prevent Disease Through Healthy DigestionNo ratings yet
- Care of The Hospitalized ChildDocument60 pagesCare of The Hospitalized ChildJSeasharkNo ratings yet
- Fundamental Pharmacology ConceptsDocument21 pagesFundamental Pharmacology ConceptsYean Delos ReyesNo ratings yet
- EndocrinedisorderDocument3 pagesEndocrinedisorderDyan LazoNo ratings yet
- Moodle 2 - Reading NewspapersDocument4 pagesMoodle 2 - Reading Newspapersvuongquynhanh120202No ratings yet
- DiPiro Section 3 - Special PopulationsDocument31 pagesDiPiro Section 3 - Special PopulationsFrisNo ratings yet
- Off-Label Drug Use in Pediatric Patients: ReviewsDocument6 pagesOff-Label Drug Use in Pediatric Patients: ReviewsRestu SNo ratings yet
- Postpartum Mood DisordersDocument33 pagesPostpartum Mood Disorderstanmai nooluNo ratings yet
- When Your Child Won’T Eat or Eats Too Much: A Parents’ Guide for the Prevention and Treatment of Feeding Problems in Young ChildrenFrom EverandWhen Your Child Won’T Eat or Eats Too Much: A Parents’ Guide for the Prevention and Treatment of Feeding Problems in Young ChildrenNo ratings yet
- Pharmacokinetics in Special PopulationsDocument26 pagesPharmacokinetics in Special PopulationsAnkita banerjeeNo ratings yet
- Failure To ThriveDocument8 pagesFailure To ThriveFitria AhdiyantiNo ratings yet
- Thesis English 4Document21 pagesThesis English 4Hermiie Joii Galang MaglaquiiNo ratings yet
- PosologyDocument30 pagesPosologyPIYUSHA NEJDARNo ratings yet
- Effects of Eating Junkfoods To The Health of The Students of Bayambang National HighschoolDocument8 pagesEffects of Eating Junkfoods To The Health of The Students of Bayambang National HighschoolFrancine Kaye BautistaNo ratings yet
- Module 2: Chapter 1 Learning ActivitiesDocument6 pagesModule 2: Chapter 1 Learning ActivitiesEloise GalsimNo ratings yet
- Nurses' Role in Drug Administration To ChildrenDocument7 pagesNurses' Role in Drug Administration To Childrenanne_ochoa100% (1)
- Pediatric DrugDocument68 pagesPediatric DrugHossen AliNo ratings yet
- Republic of The Philippines Tamag, Vigan City 2700 Ilocos SurDocument8 pagesRepublic of The Philippines Tamag, Vigan City 2700 Ilocos SurJewel Ramos GalinatoNo ratings yet
- 101 Complementary and Integrative MedicineDocument3 pages101 Complementary and Integrative MedicineAnonymous NEJodF0HXqNo ratings yet
- Pediatric Pharmacology - Dr. JangiDocument29 pagesPediatric Pharmacology - Dr. JangiBashar Khalil100% (1)
- Kee: Pharmacology, 8th Edition: Chapter 7: Pediatric Pharmacology Downloadable Key PointsDocument2 pagesKee: Pharmacology, 8th Edition: Chapter 7: Pediatric Pharmacology Downloadable Key PointsLondera BainNo ratings yet
- Pharmacology and PediatricsDocument5 pagesPharmacology and PediatricsahmedalarwaliNo ratings yet
- Posology 151223081101Document24 pagesPosology 151223081101eswarNo ratings yet
- Pharmaceutics: Factors and Mechanisms For Pharmacokinetic Differences Between Pediatric Population and AdultsDocument20 pagesPharmaceutics: Factors and Mechanisms For Pharmacokinetic Differences Between Pediatric Population and AdultsRosa Gdp GarciaNo ratings yet
- Monthly Membership Subscription FAQsDocument2 pagesMonthly Membership Subscription FAQsm1k0eNo ratings yet
- How Bankruptcy Affects Real Estate Titles and Bankruptcy Risks Covered by Title Insurance - 00104887Document11 pagesHow Bankruptcy Affects Real Estate Titles and Bankruptcy Risks Covered by Title Insurance - 00104887m1k0eNo ratings yet
- LicenseDocument7 pagesLicenseAdnan AvdukićNo ratings yet
- IV medication reconstitution checklistDocument3 pagesIV medication reconstitution checklistm1k0eNo ratings yet
- HTN - Sodium PPT EditionDocument15 pagesHTN - Sodium PPT Editionm1k0eNo ratings yet
- Hyponatremia: Symptoms May Vary With Changes in Vascular VolumeDocument3 pagesHyponatremia: Symptoms May Vary With Changes in Vascular Volumem1k0eNo ratings yet
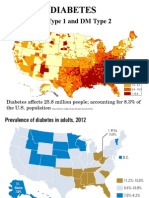
- Endo DM Type 1 and 2Document35 pagesEndo DM Type 1 and 2m1k0eNo ratings yet
- Ati Codes Cont'Document1 pageAti Codes Cont'm1k0eNo ratings yet
- Osteoarthritis, Hip Replacement, OsteoporosisDocument19 pagesOsteoarthritis, Hip Replacement, Osteoporosism1k0eNo ratings yet
- ATIpendixDocument38 pagesATIpendixm1k0e100% (1)
- ATI CollaborationDocument46 pagesATI Collaborationm1k0e72% (29)
- MGMT E-2000 Fall 2014 SyllabusDocument13 pagesMGMT E-2000 Fall 2014 Syllabusm1k0eNo ratings yet
- EKG Crash Course NuRsing 390 SMC - 4Document57 pagesEKG Crash Course NuRsing 390 SMC - 4m1k0e100% (2)
- Antimicrobial Stewardship: Attempting To Preserve A Strategic ResourceDocument7 pagesAntimicrobial Stewardship: Attempting To Preserve A Strategic Resourcem1k0eNo ratings yet
- HTN - Sodium PPT EditionDocument15 pagesHTN - Sodium PPT Editionm1k0eNo ratings yet
- Obtaining A Pap SmearDocument1 pageObtaining A Pap Smearm1k0eNo ratings yet
- Introduction To Pediatric Nursing 2012 Student VersionDocument71 pagesIntroduction To Pediatric Nursing 2012 Student Versionm1k0eNo ratings yet
- Reducing Inappropriate Antibiotic Prescribing in The Residential Care Setting: Current PerspectivesDocument13 pagesReducing Inappropriate Antibiotic Prescribing in The Residential Care Setting: Current Perspectivesm1k0eNo ratings yet
- Effectiveness of A Comprehensive Hand Hygiene Program ForDocument11 pagesEffectiveness of A Comprehensive Hand Hygiene Program Form1k0eNo ratings yet
- Medicine American Journal of Hospice and PalliativeDocument6 pagesMedicine American Journal of Hospice and Palliativem1k0eNo ratings yet
- Mus Culo Skeletal Exam OutlineDocument14 pagesMus Culo Skeletal Exam Outlinem1k0eNo ratings yet
- The Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of LifeDocument4 pagesThe Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of Lifem1k0eNo ratings yet
- Health & Physical Assessment in Nursing: Donita D'Amico Colleen BarbaritoDocument48 pagesHealth & Physical Assessment in Nursing: Donita D'Amico Colleen Barbaritom1k0eNo ratings yet
- Atoal Material Safety Data SheetsDocument1 pageAtoal Material Safety Data Sheetsm1k0eNo ratings yet
- Hesi Entrance Examination Study GuideDocument195 pagesHesi Entrance Examination Study Guidetken35100% (2)
- Guide To UspsDocument28 pagesGuide To Uspsm1k0eNo ratings yet
- Effectiveness of A Comprehensive Hand Hygiene Program ForDocument11 pagesEffectiveness of A Comprehensive Hand Hygiene Program Form1k0eNo ratings yet
- Chapter 3 Macromolecules and The Origin of LifeDocument13 pagesChapter 3 Macromolecules and The Origin of Lifem1k0eNo ratings yet
- Chapter 003Document2 pagesChapter 003m1k0eNo ratings yet
- 7211 Vitamin K 2014Document42 pages7211 Vitamin K 2014m1k0eNo ratings yet
- Updated - CHAPTER 3 Nutrition and DigestionDocument40 pagesUpdated - CHAPTER 3 Nutrition and Digestiondeela decemberNo ratings yet
- Journal of Gastro Buc 2017 InteriorDocument139 pagesJournal of Gastro Buc 2017 InteriorAnonymous CQmrhq1O7No ratings yet
- Laboratory Manual On Dissection of FrogDocument10 pagesLaboratory Manual On Dissection of FrogChadwin B. MorenteNo ratings yet
- Homeostasis 2020Document43 pagesHomeostasis 2020Godfrey Pizaroh MujuziNo ratings yet
- Liver Function Test Report for Mr. Ketan ChavanDocument1 pageLiver Function Test Report for Mr. Ketan ChavanRajaNo ratings yet
- Hepatomegaly: An Approach To Differential DiagnosisDocument14 pagesHepatomegaly: An Approach To Differential DiagnosisJose JulcaNo ratings yet
- Mirizzi Syndrome-Rare Cause of Major Biliary Complications. Case ReportDocument3 pagesMirizzi Syndrome-Rare Cause of Major Biliary Complications. Case ReportWelviraHandayaniNo ratings yet
- Banti Syndrome PDFDocument8 pagesBanti Syndrome PDFWiyosa RusdiNo ratings yet
- Hepatic Computed Tomography and Cholangiography by Use of Gadoxetic Acid in Healthy CatsDocument11 pagesHepatic Computed Tomography and Cholangiography by Use of Gadoxetic Acid in Healthy CatsAlejandro Estrada RiosNo ratings yet
- Medical Terminology CH 8Document139 pagesMedical Terminology CH 8ياسين المسطوNo ratings yet
- SS3 Biology Lesson NoteDocument64 pagesSS3 Biology Lesson Notepalmer okiemuteNo ratings yet
- Case Study Cirrhosis of LiverDocument26 pagesCase Study Cirrhosis of LiverMonika Seervi100% (1)
- GIT-III Module PDFDocument9 pagesGIT-III Module PDFFaiz MansoorNo ratings yet
- YtDocument10 pagesYthumanNo ratings yet
- Liver and GallbladderDocument2 pagesLiver and GallbladderDanielle CapangpanganNo ratings yet
- The Basics of Iridology 2 - Maps by Puerari FrancescoDocument322 pagesThe Basics of Iridology 2 - Maps by Puerari FrancescoAmit KapoorNo ratings yet
- Acute GastroenteritisDocument56 pagesAcute Gastroenteritisneil052298% (46)
- Cancer Self TreatmentDocument35 pagesCancer Self TreatmentRichard HoltNo ratings yet
- Efek Hepatoprotektor Sari Buah Wortel (Daucus Carota L.) Pada Mencit Yang Diinduksi ParasetamolDocument5 pagesEfek Hepatoprotektor Sari Buah Wortel (Daucus Carota L.) Pada Mencit Yang Diinduksi ParasetamolririnNo ratings yet
- Everything You Need to Know About Hepatitis DDocument2 pagesEverything You Need to Know About Hepatitis DYanna Habib-MangotaraNo ratings yet
- Stimulate Spleen Detox with Ailgeno Homeopathic DropsDocument3 pagesStimulate Spleen Detox with Ailgeno Homeopathic DropsAnant GomekarNo ratings yet
- The Healy Programs Full List-0001Document15 pagesThe Healy Programs Full List-0001Vikram SharmaNo ratings yet
- Coconut Oil's Powerful Health BenefitsDocument5 pagesCoconut Oil's Powerful Health Benefitspedrocorreia71% (7)
- Anaphy Notes Group 4Document21 pagesAnaphy Notes Group 4Purple BombNo ratings yet
- Repertory of Nosodes PDFDocument19 pagesRepertory of Nosodes PDFSatyendra RawatNo ratings yet
- Module 6 Digestive SystemDocument6 pagesModule 6 Digestive SystemShane GempasaoNo ratings yet
- Liver & Biliary DiseaseDocument41 pagesLiver & Biliary Diseasesaump3No ratings yet
- 10 EncephalopathyDocument18 pages10 EncephalopathyAbdullah ShiddiqNo ratings yet
- 862 1894 1 PBDocument5 pages862 1894 1 PBChristo LimbongNo ratings yet
- Ultrasonographic Anatomy of Reproductive Female LeopardDocument12 pagesUltrasonographic Anatomy of Reproductive Female LeopardSandra Clavero ClopèsNo ratings yet