You might also like
- Essential Physics of Medical ImagingDocument1,043 pagesEssential Physics of Medical Imagingyacamer95% (43)
- Fever in Infants 1-3monthsDocument9 pagesFever in Infants 1-3monthsAmit RamrattanNo ratings yet
- Burns and The Reconstructive LaderDocument70 pagesBurns and The Reconstructive LaderAmit RamrattanNo ratings yet
- Emergency Management of Pulmonary EmbolismsDocument14 pagesEmergency Management of Pulmonary EmbolismsAmit RamrattanNo ratings yet
- InfluenzaDocument106 pagesInfluenzaAmit Ramrattan100% (3)
- MANAGEMENT OF ACUTE UGI BleedDocument21 pagesMANAGEMENT OF ACUTE UGI BleedAmit RamrattanNo ratings yet
- Respiratory Distress in The NewbornDocument146 pagesRespiratory Distress in The NewbornAmit RamrattanNo ratings yet
- Antepartum HaemorrhageDocument65 pagesAntepartum HaemorrhageAmit RamrattanNo ratings yet
- IntussusceptionDocument14 pagesIntussusceptionAmit RamrattanNo ratings yet
- BioPAC+Teachers GuideDocument66 pagesBioPAC+Teachers GuideAlyssa Seeraj100% (4)
- Acute Kidney InjuryDocument19 pagesAcute Kidney InjuryAmit Ramrattan0% (1)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Virtual Lab - 1.2.2 Virtual Lab Antibiotic EffectivenessDocument4 pagesVirtual Lab - 1.2.2 Virtual Lab Antibiotic EffectivenessJustice JensenNo ratings yet
- Periodontal AbscessDocument27 pagesPeriodontal AbscessAhmed Tawfig GamalNo ratings yet
- Wiley Protocol Consumer Newsletter September 2009Document3 pagesWiley Protocol Consumer Newsletter September 2009WileyProtocolNo ratings yet
- EssayDocument16 pagesEssayLorenz Sagayaga ListaNo ratings yet
- Dr. Miswar Fattah, M.Si. Kesiapan ATLM Dalam Melakukan Swab Nasofaring Dan Orofaring Dalam Percepatan Diagnostik COVID-19. PDSPatKLIn 18072020Document41 pagesDr. Miswar Fattah, M.Si. Kesiapan ATLM Dalam Melakukan Swab Nasofaring Dan Orofaring Dalam Percepatan Diagnostik COVID-19. PDSPatKLIn 18072020Rini WidyantariNo ratings yet
- Rajiv Gandhi University of Health Sciences Exam ResultDocument1 pageRajiv Gandhi University of Health Sciences Exam ResultMD ZubairNo ratings yet
- DKA EthiopiaDocument7 pagesDKA EthiopiaBrotherhood of KryptonianNo ratings yet
- Pelvic Inflammatory Disease: Dr. Indah Meyliza, M. KesDocument13 pagesPelvic Inflammatory Disease: Dr. Indah Meyliza, M. KesIndah MeylizaNo ratings yet
- ThesisDocument58 pagesThesisSimran MáhátoNo ratings yet
- Philippine's Healthcare System During The PandemicDocument1 pagePhilippine's Healthcare System During The PandemicMaria Erica Jan MirandaNo ratings yet
- Sepsis 3Document38 pagesSepsis 3EvanNo ratings yet
- Mangialavori - 3 Remedies For COVIDDocument3 pagesMangialavori - 3 Remedies For COVIDaldodias100% (1)
- Test Bank For Health Psychology 2 e 2nd Edition Deborah Fish RaginDocument34 pagesTest Bank For Health Psychology 2 e 2nd Edition Deborah Fish RaginpudgyoverburnnggNo ratings yet
- Pakistan FloodsDocument13 pagesPakistan FloodsfashionIDM77No ratings yet
- Nepal Police SyllabusDocument12 pagesNepal Police SyllabusBinayak UpadhyayaNo ratings yet
- TuberculosisDocument4 pagesTuberculosisdreamxtreme16100% (2)
- Indian Chilhood CirrhosisDocument28 pagesIndian Chilhood CirrhosisBelbi MolNo ratings yet
- ProductsDocument65 pagesProductsanooprajguruNo ratings yet
- Tonsil Cancer: Cedars-Sinai ResourceDocument4 pagesTonsil Cancer: Cedars-Sinai ResourceSiRa DiktaraNo ratings yet
- Required Coursework For Dental SchoolDocument5 pagesRequired Coursework For Dental Schoolrqaeibifg100% (2)
- Slowther and Kleinman - ConfidentialityDocument4 pagesSlowther and Kleinman - ConfidentialitysugarmelodiesNo ratings yet
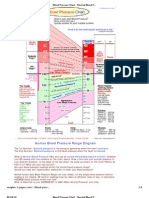
- Blood Pressure ChartDocument4 pagesBlood Pressure ChartPixelateNo ratings yet
- Client With High-RiskDocument170 pagesClient With High-RiskLongyapon Sheena Stephanie100% (2)
- Staffing ComputationsDocument24 pagesStaffing ComputationsOliric Acnab Nabcih100% (4)
- Probiotics Downloadable PDFDocument2 pagesProbiotics Downloadable PDFGreg WrightNo ratings yet
- Who Ucn GMP 2023.01 EngDocument447 pagesWho Ucn GMP 2023.01 EngSamantha BudiawanNo ratings yet
- Cardiology BrochureDocument2 pagesCardiology Brochureong251183No ratings yet
- Reseaech Group 4 1 AutoRecovered 2 1Document70 pagesReseaech Group 4 1 AutoRecovered 2 1Abegail Joy AragonNo ratings yet
- Communication Interaction in ICU-Patient and Staff Experiences and Perceptions.Document5 pagesCommunication Interaction in ICU-Patient and Staff Experiences and Perceptions.osondoarNo ratings yet
- Hypertension and Herbal Plant For Its Treatment: A ReviewDocument1 pageHypertension and Herbal Plant For Its Treatment: A Reviewdyan ayu puspariniNo ratings yet