You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- List of Mineral Function and DeficiencyDocument16 pagesList of Mineral Function and Deficiencyketavmodi100% (8)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- School of Out-Of-BodyDocument224 pagesSchool of Out-Of-Bodyrpandit075698100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Pathoma, Sketchy Pharm & Micro, B&B Video TimesDocument52 pagesPathoma, Sketchy Pharm & Micro, B&B Video TimesAlina PolancoNo ratings yet
- Summer Training For Speed: Alwyn Cosgrove's Training Design ProgramDocument6 pagesSummer Training For Speed: Alwyn Cosgrove's Training Design ProgramSteve HeywoodNo ratings yet
- Endocrine and Metabolic Disorders PDFDocument31 pagesEndocrine and Metabolic Disorders PDFAna-Maria50% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Iron Deficiency Anaemia in Toddlers: Learning PointsDocument8 pagesIron Deficiency Anaemia in Toddlers: Learning PointsAfiqah So JasmiNo ratings yet
- Heat Stress Management Training ProgramDocument28 pagesHeat Stress Management Training ProgramDheeraj Dheeru100% (1)
- Operating RoomDocument81 pagesOperating Roomjaypee01100% (3)
- Endocrine Glands RevisedDocument47 pagesEndocrine Glands RevisedXyress Archer GosinganNo ratings yet
- Anatomy of Long Bone and Classification of Joints: Prepared by DR Dipendra Maharjan 1 Yr Resident, NAMSDocument32 pagesAnatomy of Long Bone and Classification of Joints: Prepared by DR Dipendra Maharjan 1 Yr Resident, NAMSAfiqah So JasmiNo ratings yet
- Growth Charts For Children With Down Syndrome CanDocument12 pagesGrowth Charts For Children With Down Syndrome CanAfiqah So JasmiNo ratings yet
- Imm 922Document1 pageImm 922Afiqah So JasmiNo ratings yet
- Summary of New Recommendations: HIV Testing and CounsellingDocument9 pagesSummary of New Recommendations: HIV Testing and CounsellingAfiqah So JasmiNo ratings yet
- Growth Charts For Down's Syndrome From Birth To 18 Years of AgeDocument7 pagesGrowth Charts For Down's Syndrome From Birth To 18 Years of AgeAfiqah So JasmiNo ratings yet
- Barb Melo SkyDocument17 pagesBarb Melo SkyAfiqah So JasmiNo ratings yet
- Pathophysiology Infants: of inDocument4 pagesPathophysiology Infants: of inAfiqah So JasmiNo ratings yet
- CI Mar2012 Growth Charts en - Rev2013Document13 pagesCI Mar2012 Growth Charts en - Rev2013Afiqah So JasmiNo ratings yet
- Theories OutlineDocument16 pagesTheories Outlineapi-242756158No ratings yet
- Improve Your Hands-On Nutrition Physical Exam SkillsDocument27 pagesImprove Your Hands-On Nutrition Physical Exam SkillsAfiqah So JasmiNo ratings yet
- Overview07 WebDocument34 pagesOverview07 WebAfiqah So JasmiNo ratings yet
- Catalysis Experiment 6Document4 pagesCatalysis Experiment 6Marianne Rose HernandezNo ratings yet
- Questions & Answers: For For For For For NEET (UG) - 2020Document21 pagesQuestions & Answers: For For For For For NEET (UG) - 2020Ritu JoharNo ratings yet
- Tseng Chromosome Analysis PDFDocument24 pagesTseng Chromosome Analysis PDFLouie AndersonNo ratings yet
- Cell Membranes and Transport TestDocument3 pagesCell Membranes and Transport Testapi-252516966No ratings yet
- Resp AssessmentDocument19 pagesResp AssessmentNURSES- NOOK & CORNERNo ratings yet
- Proteolytic Enzyme: Basic Information and Cleavage Rules: Dr. Aditya AryaDocument11 pagesProteolytic Enzyme: Basic Information and Cleavage Rules: Dr. Aditya Aryaabcxyz7799No ratings yet
- Chapter 24)Document10 pagesChapter 24)Hazel LopezNo ratings yet
- Gout CPG Manuscript - PJIM 072808Document16 pagesGout CPG Manuscript - PJIM 072808Francis CastellNo ratings yet
- Bloody Tears Following Lefort 1Document3 pagesBloody Tears Following Lefort 1paulwhite1234No ratings yet
- And Um-101Document3 pagesAnd Um-101ver_at_workNo ratings yet
- Examen de Bioquimica PDFDocument11 pagesExamen de Bioquimica PDFNicolás BeltránNo ratings yet
- Summative Test-G8-Quarter-4Document13 pagesSummative Test-G8-Quarter-4Charmaine CanonoNo ratings yet
- 11 Biology Notes ch05 Morphology of Flowering Plants PDFDocument7 pages11 Biology Notes ch05 Morphology of Flowering Plants PDFMeenakshi VenkataramanNo ratings yet
- Cardio CaseDocument21 pagesCardio CaseJan Rae Y. BattungNo ratings yet
- Eng 103Document253 pagesEng 103CArmina Reyes Gajo0% (1)
- OB Case StudyDocument18 pagesOB Case StudyPramod A.NNo ratings yet
- Encoding: Cognitive Perspective: Fergus I. M. .CraikDocument9 pagesEncoding: Cognitive Perspective: Fergus I. M. .Craikambar tri wahyuniNo ratings yet
- Technique Used For Study of Bio Synthetic PathwayDocument9 pagesTechnique Used For Study of Bio Synthetic Pathwayshankul kumar95% (19)
- Transcript of RecordsDocument3 pagesTranscript of Recordsmi5agencyNo ratings yet
- 1.4 Selecton of Blood BagDocument3 pages1.4 Selecton of Blood BagBALAJINo ratings yet
- Progr. PR., Simpozion Boli Genet Metab, Cluj-Napoca, 7-8 IunieDocument3 pagesProgr. PR., Simpozion Boli Genet Metab, Cluj-Napoca, 7-8 IunieDoina Ababii UrsanNo ratings yet
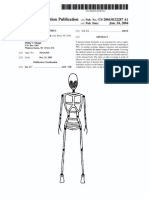
- Patente Endoesqueleto para Sex Doll SiliconaDocument12 pagesPatente Endoesqueleto para Sex Doll SiliconaGabriel De Jesus100% (1)