You might also like
- Inflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandInflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Asthma Training Module 2013Document204 pagesAsthma Training Module 2013Carlo AlvaradoNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanGabrielGitaNo ratings yet
- 12 Cranial NervesDocument1 page12 Cranial Nervesadrianne30No ratings yet
- Acute Bronchiolitis EditedDocument19 pagesAcute Bronchiolitis EditedSurgicalgownNo ratings yet
- Pneumonia and BronchiolitisDocument48 pagesPneumonia and Bronchiolitisshashank panwarNo ratings yet
- Respiratory System MedicationsDocument2 pagesRespiratory System Medicationsmlbrown8No ratings yet
- NRSG 115 CCL CDL Spring 2020 Lab Information SheetDocument7 pagesNRSG 115 CCL CDL Spring 2020 Lab Information SheetSethNo ratings yet
- 406 - Respiratory Therapy Consult Service HandbookDocument28 pages406 - Respiratory Therapy Consult Service HandbookIkhsan JohnsonNo ratings yet
- Childhood AsthmaDocument40 pagesChildhood AsthmachinchuNo ratings yet
- Respiratory Care ModalitiesDocument63 pagesRespiratory Care ModalitiesErica Clerigo LandichoNo ratings yet
- Expanded 3P Study Guide YasminaIrinaDocument79 pagesExpanded 3P Study Guide YasminaIrinaikNo ratings yet
- VSim SARAH LIN For Nursing - Health Assessment POST QUIZDocument5 pagesVSim SARAH LIN For Nursing - Health Assessment POST QUIZWen RodsaNo ratings yet
- Registered Respiratory TherapistDocument3 pagesRegistered Respiratory Therapistapi-76909521No ratings yet
- If Symptoms Are Not Recognized and Treated in A Timely Manner, Complications That CharlieDocument5 pagesIf Symptoms Are Not Recognized and Treated in A Timely Manner, Complications That Charliesalman ahmedNo ratings yet
- Registry Examination For Advanced Respiratory Therapists (RRT)Document6 pagesRegistry Examination For Advanced Respiratory Therapists (RRT)Sandy HartmanNo ratings yet
- COPD Acute Management ABCDEDocument11 pagesCOPD Acute Management ABCDESSNo ratings yet
- Health History AssignmentDocument6 pagesHealth History AssignmentgeegundelyNo ratings yet
- Respiratory Therapist, NICU/ICUDocument5 pagesRespiratory Therapist, NICU/ICUapi-77517256No ratings yet
- RT 220 B C AirwaystudyguideDocument25 pagesRT 220 B C Airwaystudyguiderpebdani0% (2)
- Chest Pain System - DisorderDocument1 pageChest Pain System - DisorderAA DDNo ratings yet
- Laboratory Examinations: Allen's Test Normal Finding: Hand Quickly BecomesDocument9 pagesLaboratory Examinations: Allen's Test Normal Finding: Hand Quickly BecomesShane GumaponNo ratings yet
- PAT - Remick Spring CE 2014Document50 pagesPAT - Remick Spring CE 2014Nadar RizatullahNo ratings yet
- Chronic BronchitisDocument2 pagesChronic BronchitisEimhie Lee CasiNo ratings yet
- Module 8 - Physical AssessmentDocument10 pagesModule 8 - Physical AssessmentPaulette Poseskie CoatesNo ratings yet
- Pulmonary Function Test, JARA CSUDocument73 pagesPulmonary Function Test, JARA CSUJohn NicoleNo ratings yet
- Respiratory Management in Pediatrics PDFDocument68 pagesRespiratory Management in Pediatrics PDFPAKINUGNo ratings yet
- Patho Exam 3: Deficiency in Alpha-1-Antitrypsin-Unchecked Elastase Destruction of The AlveoliDocument5 pagesPatho Exam 3: Deficiency in Alpha-1-Antitrypsin-Unchecked Elastase Destruction of The AlveoliTaran LuthraNo ratings yet
- Patient Care SkillsDocument15 pagesPatient Care SkillsIts John100% (1)
- Pediatric AsthmaDocument2 pagesPediatric AsthmaAntonio TayaoNo ratings yet
- Ards PedDocument26 pagesArds PedGustavo OlguinNo ratings yet
- 8 Lung Auscultation Points and SoundsDocument11 pages8 Lung Auscultation Points and SoundsCHARIEMAE CA�AZARES100% (1)
- Lower Respiratory Tract Diseases - KeyDocument45 pagesLower Respiratory Tract Diseases - KeyYugmaPandyaNo ratings yet
- 10 Oropharyngeal and Nasopharyngeal SuctioningDocument8 pages10 Oropharyngeal and Nasopharyngeal SuctioningKen Morales Alcantara100% (1)
- ARDSDocument27 pagesARDSChloie Marie RosalejosNo ratings yet
- Mechanical Ventilation and Intracranial PressureDocument30 pagesMechanical Ventilation and Intracranial PressureFlavius AnghelNo ratings yet
- Adventitious Breath SoundsDocument1 pageAdventitious Breath SoundsEdwin Delos Reyes AbuNo ratings yet
- Infectious Disease MedicationsDocument8 pagesInfectious Disease MedicationsSheril MarekNo ratings yet
- Lower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument95 pagesLower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingRI NANo ratings yet
- Head To Toe AssessmentDocument22 pagesHead To Toe AssessmentNessa Layos MorilloNo ratings yet
- SBAR WorksheetDocument3 pagesSBAR Worksheet6bigstar9No ratings yet
- Case Study Bronchial-AsthmaDocument9 pagesCase Study Bronchial-AsthmaGabbii CincoNo ratings yet
- ' PDFDocument1 page' PDFmp1757No ratings yet
- Respiratory Care Standard Abbreviations and SymbolsDocument6 pagesRespiratory Care Standard Abbreviations and SymbolsHussein FatalNo ratings yet
- Asthma Action PlanDocument2 pagesAsthma Action PlanCharles S. Williams RRT, AE-CNo ratings yet
- Noninvasive VentilationDocument6 pagesNoninvasive VentilationEma MagfirahNo ratings yet
- Assessment of The Chest and LungsDocument46 pagesAssessment of The Chest and LungsSumathi GopinathNo ratings yet
- Health Effects of Secondhand SmokeDocument4 pagesHealth Effects of Secondhand SmokeCris Tarrazona CasipleNo ratings yet
- Asthma MimickersDocument6 pagesAsthma MimickersHarpreet SinghNo ratings yet
- Completed Concept MapDocument4 pagesCompleted Concept Mapapi-607361848No ratings yet
- Normal Breath SoundsDocument1 pageNormal Breath Soundsyanks1120No ratings yet
- Lab Test GuideDocument28 pagesLab Test GuideNica Paredes MiravallesNo ratings yet
- Oxygenation NCM 103Document10 pagesOxygenation NCM 103Richmond LacadenNo ratings yet
- NCPDocument3 pagesNCPFaye Spring TravillaNo ratings yet
- Shortness of BreathDocument17 pagesShortness of BreathChingHuaNo ratings yet
- StrokeDocument1 pageStrokeMariel Febreo MerlanNo ratings yet
- Bates' Visual Guide To Physical Examination Vol. 7: Head, Eyes, and EarsDocument9 pagesBates' Visual Guide To Physical Examination Vol. 7: Head, Eyes, and EarsArlene DaroNo ratings yet
- Respiratory EmergenciesDocument34 pagesRespiratory EmergenciesRoshana MallawaarachchiNo ratings yet
- Critical Event Checklists PDFDocument27 pagesCritical Event Checklists PDFMateas ZsoltNo ratings yet
- Inhaled Nitric OxideDocument24 pagesInhaled Nitric OxidesajaNo ratings yet
- Ant-Man and The WaspDocument147 pagesAnt-Man and The WaspDr_Bhavesh_ParmarNo ratings yet
- Category Type of Contact Recommended TreatmentDocument1 pageCategory Type of Contact Recommended TreatmentDr_Bhavesh_ParmarNo ratings yet
- TodoDocument1 pageTodoDr_Bhavesh_ParmarNo ratings yet
- Asthma Training Module - 2013Document204 pagesAsthma Training Module - 2013Dr_Bhavesh_ParmarNo ratings yet
- WHO Guideline On Acceptable Medical Reasons For Use of Breast-Milk SubstitutesDocument12 pagesWHO Guideline On Acceptable Medical Reasons For Use of Breast-Milk SubstitutesMedarabiaNo ratings yet
- Drugs Acting On Respiratory SystemDocument3 pagesDrugs Acting On Respiratory SystemAlyssa Audrey CaoagasNo ratings yet
- Cipla Limited Vs Novartis AppellantDocument11 pagesCipla Limited Vs Novartis AppellantUNIVERSITY LAW COLLEGE BHUBANESWARNo ratings yet
- Ian Govias Gaynor Mitchell - Asthma Education Principles and Practice For The Asthma Educator.-Springer Nature (2021)Document660 pagesIan Govias Gaynor Mitchell - Asthma Education Principles and Practice For The Asthma Educator.-Springer Nature (2021)Алина КостюковаNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlannamitaNo ratings yet
- Duavent Drug Study - CunadoDocument3 pagesDuavent Drug Study - CunadoLexa Moreene Cu�adoNo ratings yet
- Nursing Practice III EdgeworthDocument8 pagesNursing Practice III EdgeworthRichard Ines Valino100% (5)
- Konno 2014Document10 pagesKonno 2014Sridevi AnggrainiNo ratings yet
- Clinical, Spirometric and Therapeutic Profil of Frequent Exacerbators in COPDDocument1 pageClinical, Spirometric and Therapeutic Profil of Frequent Exacerbators in COPDEddy FriguiNo ratings yet
- Bronchial AsthmaDocument3 pagesBronchial AsthmakiLLingspErmNo ratings yet
- Teaching Slide Set 2019: Global Initiative For Chronic Obstructive Lung Disease (Gold)Document135 pagesTeaching Slide Set 2019: Global Initiative For Chronic Obstructive Lung Disease (Gold)zaimmuhtar100% (1)
- NCLEX Questions PulmDocument27 pagesNCLEX Questions PulmAnthony Hawley100% (2)
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument16 pagesPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNo ratings yet
- Resp TestDocument7 pagesResp TestKong KongNo ratings yet
- Cipla Limited Vs Novartis Appellant PDFDocument11 pagesCipla Limited Vs Novartis Appellant PDFUNIVERSITY LAW COLLEGE BHUBANESWARNo ratings yet
- Consenso Chileno Sochinep-Ser para El Diagnostico y Tratamiento Del Asma en El EscolarDocument21 pagesConsenso Chileno Sochinep-Ser para El Diagnostico y Tratamiento Del Asma en El EscolarCONSTANZA VICTORIA QUIJADANo ratings yet
- Care of Patients On Lower Respiratory System Drugs Presented by Donnahae Rhoden SalmonDocument39 pagesCare of Patients On Lower Respiratory System Drugs Presented by Donnahae Rhoden SalmonKishi CopelandNo ratings yet
- Pulmonary Pharmacology Anticoughing AgentsDocument10 pagesPulmonary Pharmacology Anticoughing AgentsanaNo ratings yet
- Nebulized Epinephrine For Croup in Children (Review) : CochraneDocument17 pagesNebulized Epinephrine For Croup in Children (Review) : Cochranesyepri AnnaNo ratings yet
- Lesson 5 - Respiratory DrugsDocument69 pagesLesson 5 - Respiratory DrugsMarc AndrewNo ratings yet
- Drug StudyDocument4 pagesDrug Studyreanne_davidNo ratings yet
- 9 18 Trelegy Ellipta Media Factsheet Final Approved 2Document3 pages9 18 Trelegy Ellipta Media Factsheet Final Approved 2Peter GálvezNo ratings yet
- Asthma MedicationDocument6 pagesAsthma Medicationmomina arshidNo ratings yet
- Drugs Acting On Respiratory SystemDocument15 pagesDrugs Acting On Respiratory SystemQusai BassamNo ratings yet
- DS SalbutamolDocument1 pageDS SalbutamolLarr SumalpongNo ratings yet
- Doxophylline Prescribing InformationDocument1 pageDoxophylline Prescribing InformationMohammed shamiul ShahidNo ratings yet
- 7081 - PHARMA - AnnualReport - 2001-12-31 - Pharma-OpsActivities-Achievements (795KB) - 583228015Document35 pages7081 - PHARMA - AnnualReport - 2001-12-31 - Pharma-OpsActivities-Achievements (795KB) - 583228015surayaNo ratings yet
- Brodil LevoDocument2 pagesBrodil LevoAziza KhairunNo ratings yet
- Lab 9 RespitatoryDocument3 pagesLab 9 RespitatoryanaNo ratings yet
- NCM 106 Learning Activities (Semis)Document12 pagesNCM 106 Learning Activities (Semis)Kimberly Abellar LatoNo ratings yet
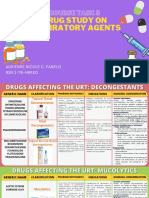
- Course Task 8 Drug Study On Respiratory AgentsDocument23 pagesCourse Task 8 Drug Study On Respiratory AgentsAdrienne Nicole PaneloNo ratings yet