You might also like
- CCRN Review Part 1: "Never Let What You Cannot Do Interfere With What You Can Do"Document160 pagesCCRN Review Part 1: "Never Let What You Cannot Do Interfere With What You Can Do"Paolo VegaNo ratings yet
- CCRN Review Course 2015Document81 pagesCCRN Review Course 2015Michelle LindsayNo ratings yet
- CCRN EexamhandbookDocument30 pagesCCRN EexamhandbookBahaa Ahmad Assoud100% (2)
- CCRN-PCCN-CMC Review Cardiac Part 1 PDFDocument14 pagesCCRN-PCCN-CMC Review Cardiac Part 1 PDFGiovanni Mictil100% (1)
- CCRN Exam CramDocument2 pagesCCRN Exam CramJan Marcus0% (3)
- CCRNDocument17 pagesCCRNNílo Stárn100% (1)
- CCRN CardiacDocument39 pagesCCRN CardiacMike100% (5)
- Endocrine, Neuro, and GI Review for Nursing ExamDocument19 pagesEndocrine, Neuro, and GI Review for Nursing ExamMelissaDavis67% (6)
- Cardiovascular Certification Review: Cardiogenic Shock, Cardiac Tamponade and MoreDocument18 pagesCardiovascular Certification Review: Cardiogenic Shock, Cardiac Tamponade and MoreGiovanni MictilNo ratings yet
- CCRN Synergy and Exam StartegiesDocument12 pagesCCRN Synergy and Exam StartegiesMarcus, RN100% (2)
- 409 Pope, B. and Maillie, S. CCRN-PCCN Review Multisystem and Q and ADocument21 pages409 Pope, B. and Maillie, S. CCRN-PCCN Review Multisystem and Q and Agliftan100% (2)
- CCRN Sample QuestionsDocument5 pagesCCRN Sample Questionsgwapdose50% (2)
- 209 Pope, B. CCRN-PCCN-CMC Review Cardiac Part 1Document14 pages209 Pope, B. CCRN-PCCN-CMC Review Cardiac Part 1peanant100% (1)
- Pope, B. CCRN-PCCN-CMC Review Endocrine and BehavioralDocument14 pagesPope, B. CCRN-PCCN-CMC Review Endocrine and BehavioralKeisha JenkinsNo ratings yet
- CCRN PulmonaryDocument107 pagesCCRN PulmonaryCzarina Charmaine Diwa100% (4)
- CCRN-PCCN-CMC Review Cardiac Part 2Document21 pagesCCRN-PCCN-CMC Review Cardiac Part 2Giovanni Mictil100% (1)
- CCRN-PCCN Review GastrointestinalDocument23 pagesCCRN-PCCN Review GastrointestinalGiovanni MictilNo ratings yet
- Icu Nursing BrainDocument2 pagesIcu Nursing Brainapi-282417591100% (2)
- 8 Week CCRN Study PlanDocument6 pages8 Week CCRN Study PlanJoshua Atienza100% (2)
- CCRN ReviewDocument22 pagesCCRN ReviewMelissaDavis71% (7)
- Hemodynamic Assessment ParametersDocument2 pagesHemodynamic Assessment ParametersalexNo ratings yet
- CCRN Cert Review Neuro IDocument16 pagesCCRN Cert Review Neuro IGiovanni MictilNo ratings yet
- Hemodynamic Management Pocket Card PDFDocument8 pagesHemodynamic Management Pocket Card PDFjenn1722No ratings yet
- Critical Care Nursing Certification: Springhouse Review ForDocument384 pagesCritical Care Nursing Certification: Springhouse Review ForNrhildaNo ratings yet
- Boot Camp Hemodynamic MonitoringDocument37 pagesBoot Camp Hemodynamic MonitoringTinaHo100% (7)
- CNEA - CCRN Review - Behavioral-PsychosocialDocument12 pagesCNEA - CCRN Review - Behavioral-PsychosocialalexNo ratings yet
- CCRN-PCCN Review RenalDocument11 pagesCCRN-PCCN Review RenalGiovanni MictilNo ratings yet
- Adult CCRN Exam Premium: For the Latest Exam Blueprint, Includes 3 Practice Tests, Comprehensive Review, and Online Study PrepFrom EverandAdult CCRN Exam Premium: For the Latest Exam Blueprint, Includes 3 Practice Tests, Comprehensive Review, and Online Study PrepNo ratings yet
- ACAQ Crit Care Nursing CurriculumDocument91 pagesACAQ Crit Care Nursing CurriculumAnne Julia Agustin100% (1)
- CCRN Cert Review Neuro 2Document15 pagesCCRN Cert Review Neuro 2Giovanni MictilNo ratings yet
- Dysrhythmia Recognition Pocket Reference Card PDFDocument14 pagesDysrhythmia Recognition Pocket Reference Card PDFjenn1722100% (2)
- Pharmacological Tools: Doses, Routes, and Uses of Common DrugDocument1 pagePharmacological Tools: Doses, Routes, and Uses of Common DrugApuntesdemedicinaa blogNo ratings yet
- ACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationDocument75 pagesACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationpolelNo ratings yet
- Cardiac NursingDocument26 pagesCardiac Nursingjgcriste95% (20)
- TNCC Prep Packet Revised June 2016Document12 pagesTNCC Prep Packet Revised June 2016nurse2012100% (3)
- CCRN AACN PremiumQs PDF PDFDocument70 pagesCCRN AACN PremiumQs PDF PDFTracy Pope100% (2)
- Adult CCRN Exam Flashcards, Second Edition: Up-to-Date Review and PracticeFrom EverandAdult CCRN Exam Flashcards, Second Edition: Up-to-Date Review and PracticeRating: 5 out of 5 stars5/5 (1)
- FLASH CardsDocument3 pagesFLASH Cardsclarheena100% (2)
- Critical Care Notes BookDocument142 pagesCritical Care Notes BookDerick RanaNo ratings yet
- Role of Critical Care Nurses in Caring for Critically Ill PatientsDocument10 pagesRole of Critical Care Nurses in Caring for Critically Ill PatientsHanis Rozib99% (69)
- PCCN PrepDocument133 pagesPCCN Prepdaniel100% (2)
- Cardiac Notes NursingDocument16 pagesCardiac Notes NursingYemaya8494% (17)
- Basic EKG Dysrhythmia IdentificationDocument40 pagesBasic EKG Dysrhythmia IdentificationIlda Dhe Devis Spaho100% (1)
- CEN+Online+Review Module+12 Final GENITODocument26 pagesCEN+Online+Review Module+12 Final GENITOTamara Cooper67% (3)
- ECMO Monitoring - PediatrikDocument24 pagesECMO Monitoring - PediatrikIsran IsRanNo ratings yet
- Critical Care - Hemodynamic Monitoring TableDocument7 pagesCritical Care - Hemodynamic Monitoring TableVictoria Romero100% (2)
- ACLS EKG Rhythms and InterpretationDocument10 pagesACLS EKG Rhythms and Interpretationdonheyzz_02No ratings yet
- Farmakologi ICUDocument54 pagesFarmakologi ICULin Phoponk100% (2)
- HemodynamicsDocument2 pagesHemodynamicsbecksterbooNo ratings yet
- Increased Intracranial Pressure and Monitoring Site PDFDocument21 pagesIncreased Intracranial Pressure and Monitoring Site PDFSari RakhmawatiNo ratings yet
- Icu NotesDocument47 pagesIcu NotesChryst Louise SaavedraNo ratings yet
- 2018 Book NursingInCriticalCareSetting PDFDocument532 pages2018 Book NursingInCriticalCareSetting PDFAnton HerdiansyahNo ratings yet
- Critical Care NursingDocument159 pagesCritical Care NursingJoy Jarin50% (2)
- Schaum's Outline of Critical Care Nursing: 250 Review QuestionsFrom EverandSchaum's Outline of Critical Care Nursing: 250 Review QuestionsRating: 5 out of 5 stars5/5 (1)
- Ccrn Certification Examination Practice Questions and Answers with Rationale: First EditionFrom EverandCcrn Certification Examination Practice Questions and Answers with Rationale: First EditionRating: 5 out of 5 stars5/5 (1)
- Thinking - NursingDocument456 pagesThinking - NursingNatalie Borisenko100% (3)
- Congestive Heart Failure LectureDocument29 pagesCongestive Heart Failure LecturePaolo VegaNo ratings yet
- AppD LAPrehospitalStrokeScreenDocument1 pageAppD LAPrehospitalStrokeScreenPaolo VegaNo ratings yet
- Philo Req MSNDocument2 pagesPhilo Req MSNPaolo VegaNo ratings yet
- APA Writing StyleDocument37 pagesAPA Writing Styleghayyur100% (10)
- CNL Role in Reducing ICU EVD InfectionsDocument35 pagesCNL Role in Reducing ICU EVD InfectionsPaolo VegaNo ratings yet
- Outline of A Research ReportDocument4 pagesOutline of A Research ReportPaolo VegaNo ratings yet
- Questions For DiscussionDocument2 pagesQuestions For DiscussionPaolo VegaNo ratings yet
- Beacon HandbookDocument30 pagesBeacon HandbookPaolo VegaNo ratings yet
- Clinical Practice Council ArticleDocument13 pagesClinical Practice Council ArticlePaolo VegaNo ratings yet
- Philo Statement 2Document9 pagesPhilo Statement 2Paolo VegaNo ratings yet
- LeadershipDocument25 pagesLeadershipfoglaabhishekNo ratings yet
- 30 Team-Building Games, Activities, and Ideas: 1. The Game of PossibilitiesDocument23 pages30 Team-Building Games, Activities, and Ideas: 1. The Game of PossibilitiesSrihari VenugopalNo ratings yet
- 130300-Standards For Acute and Critical Care NursingDocument12 pages130300-Standards For Acute and Critical Care Nursingapi-315277523No ratings yet
- Medication Errors:: Don't Let Them Happen To YouDocument6 pagesMedication Errors:: Don't Let Them Happen To YouPhuong Tran100% (1)
- The Vision The Heart The Will To ServeDocument1 pageThe Vision The Heart The Will To ServePaolo VegaNo ratings yet
- Accraopinion of CWWDocument4 pagesAccraopinion of CWWPaolo VegaNo ratings yet
- Philosophy of Education MSN-2Document37 pagesPhilosophy of Education MSN-2Paolo VegaNo ratings yet
- CNL Role in Reducing ICU EVD InfectionsDocument35 pagesCNL Role in Reducing ICU EVD InfectionsPaolo VegaNo ratings yet
- Introduction To Patient Safety Analysis and Event ManagementDocument71 pagesIntroduction To Patient Safety Analysis and Event ManagementPaolo VegaNo ratings yet
- Medication Errors Improving Practices and Patient SafetyDocument22 pagesMedication Errors Improving Practices and Patient SafetyPaolo VegaNo ratings yet
- ATLS 8th EditionDocument50 pagesATLS 8th EditionPaolo VegaNo ratings yet
- Apply CuspDocument26 pagesApply CuspPaolo VegaNo ratings yet
- Introduction To ShockDocument56 pagesIntroduction To ShockPaolo VegaNo ratings yet
- Linking Hospital Managers To LiteratureDocument32 pagesLinking Hospital Managers To LiteraturePaolo VegaNo ratings yet
- Vasoactive Agents in Emergency CareDocument46 pagesVasoactive Agents in Emergency CarePaolo VegaNo ratings yet
- Eb PN LectureDocument54 pagesEb PN LecturePaolo VegaNo ratings yet
- Introduction To ShockDocument56 pagesIntroduction To ShockPaolo VegaNo ratings yet
- Evaluating The Impact of Color Normalization On Kidney Image SegmentationDocument13 pagesEvaluating The Impact of Color Normalization On Kidney Image SegmentationJames MorenoNo ratings yet
- Tubular Reabsorption and SecretionDocument29 pagesTubular Reabsorption and SecretionenriNo ratings yet
- Cilostazol-Induced Acute Kidney Injury in A Patient WithDocument4 pagesCilostazol-Induced Acute Kidney Injury in A Patient WithjharyNo ratings yet
- SCIT 1408 Applied Human Anatomy and Physiology II - Urinary System Chapter 25 BDocument50 pagesSCIT 1408 Applied Human Anatomy and Physiology II - Urinary System Chapter 25 BChuongNo ratings yet
- Clinical Presentation On HemodialysisDocument37 pagesClinical Presentation On HemodialysisSanvar Mal SoniNo ratings yet
- Congenital Malformations and Chromosomal AbnormalitiesDocument17 pagesCongenital Malformations and Chromosomal AbnormalitiesDitta Nur apriantyNo ratings yet
- Demonstration Urine AnlysisDocument7 pagesDemonstration Urine Anlysisamit100% (1)
- Case Study On Chronic Kidney Disease Probably To Secondary HypertensionDocument18 pagesCase Study On Chronic Kidney Disease Probably To Secondary Hypertensionkyeria77% (26)
- Acid-Base Balance and DisodersDocument86 pagesAcid-Base Balance and DisodersPrincewill SeiyefaNo ratings yet
- Case Study On Kidney StoneDocument36 pagesCase Study On Kidney Stonemanojkumar200624No ratings yet
- The Kidney, Excretion and OsmoregulationDocument63 pagesThe Kidney, Excretion and OsmoregulationJfoxx SamuelNo ratings yet
- Urogenital Imejing: DR - Ali Imran Lubis SP - RadDocument16 pagesUrogenital Imejing: DR - Ali Imran Lubis SP - RadPutri Sari SeptirianiNo ratings yet
- hsns270 Assignment 1 Bhima Devi Poudel Adhikari CKD 220179000Document12 pageshsns270 Assignment 1 Bhima Devi Poudel Adhikari CKD 220179000api-525310113No ratings yet
- Fraser's GAMSAT Free Practice Test QuestionsDocument20 pagesFraser's GAMSAT Free Practice Test QuestionsVerity ShawcrossNo ratings yet
- Kidney Cancer: By: Myra R. Abria & Karen HingadaDocument33 pagesKidney Cancer: By: Myra R. Abria & Karen Hingadamynoidanh19No ratings yet
- Best Practices For Sample Storage UrineDocument41 pagesBest Practices For Sample Storage UrinekinnusaraiNo ratings yet
- Solicitation For ShannDocument4 pagesSolicitation For ShannqwertyNo ratings yet
- Acute Kidney Injury and Chronic Kidney DiseaseDocument59 pagesAcute Kidney Injury and Chronic Kidney Diseasesho bartNo ratings yet
- CKD EsrdDocument83 pagesCKD EsrdRita Lakhani100% (1)
- Circulatory System TurtleDocument32 pagesCirculatory System TurtleVillamorchardNo ratings yet
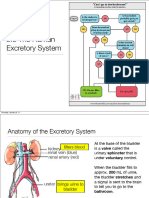
- SBI4U Unit 4 Homeostasis Excretory SystemDocument27 pagesSBI4U Unit 4 Homeostasis Excretory System전채연No ratings yet
- QP 3 PDFDocument780 pagesQP 3 PDFAliMushtaq100% (1)
- Introduction To ElectrolytesDocument13 pagesIntroduction To ElectrolytesMaam ShaNo ratings yet
- Effects of Dietary Protein Intake On Renal FunctionDocument6 pagesEffects of Dietary Protein Intake On Renal FunctiongabrielwerneckNo ratings yet
- Med Surg Study GuideDocument98 pagesMed Surg Study Guideprogramgrabber100% (23)
- Renal UltrasoundDocument179 pagesRenal UltrasoundJuhar AhamedNo ratings yet
- AKIDocument23 pagesAKInadddNo ratings yet
- Hormonal Regulation of ExerciseDocument11 pagesHormonal Regulation of ExerciseMozil Fadzil KamarudinNo ratings yet
- Understanding Drug InteractionsDocument40 pagesUnderstanding Drug Interactionsdevaky paramasivanNo ratings yet
- Yoga ICSEDocument6 pagesYoga ICSESNo ratings yet