You might also like
- APA Writing StyleDocument37 pagesAPA Writing Styleghayyur100% (10)
- Thinking - NursingDocument456 pagesThinking - NursingNatalie Borisenko100% (3)
- Congestive Heart Failure LectureDocument29 pagesCongestive Heart Failure LecturePaolo VegaNo ratings yet
- Ann Deerhake, MS, RN, CNL, CCRN: CNL USF Conference Logo 2011Document35 pagesAnn Deerhake, MS, RN, CNL, CCRN: CNL USF Conference Logo 2011Paolo VegaNo ratings yet
- Outline of A Research ReportDocument4 pagesOutline of A Research ReportPaolo VegaNo ratings yet
- AppD LAPrehospitalStrokeScreenDocument1 pageAppD LAPrehospitalStrokeScreenPaolo VegaNo ratings yet
- Medication Errors:: Don't Let Them Happen To YouDocument6 pagesMedication Errors:: Don't Let Them Happen To YouPhuong Tran100% (1)
- Questions For DiscussionDocument2 pagesQuestions For DiscussionPaolo VegaNo ratings yet
- Philo Req MSNDocument2 pagesPhilo Req MSNPaolo VegaNo ratings yet
- Clinical Practice Council ArticleDocument13 pagesClinical Practice Council ArticlePaolo VegaNo ratings yet
- 130300-Standards For Acute and Critical Care NursingDocument12 pages130300-Standards For Acute and Critical Care Nursingapi-315277523No ratings yet
- ATLS 8th EditionDocument50 pagesATLS 8th EditionPaolo VegaNo ratings yet
- Philo Statement 2Document9 pagesPhilo Statement 2Paolo VegaNo ratings yet
- 30 Team-Building Games, Activities, and Ideas: 1. The Game of PossibilitiesDocument23 pages30 Team-Building Games, Activities, and Ideas: 1. The Game of PossibilitiesSrihari VenugopalNo ratings yet
- The Vision The Heart The Will To ServeDocument1 pageThe Vision The Heart The Will To ServePaolo VegaNo ratings yet
- LeadershipDocument25 pagesLeadershipfoglaabhishekNo ratings yet
- Accraopinion of CWWDocument4 pagesAccraopinion of CWWPaolo VegaNo ratings yet
- Medication Errors Improving Practices and Patient SafetyDocument22 pagesMedication Errors Improving Practices and Patient SafetyPaolo VegaNo ratings yet
- Introduction To Patient Safety Analysis and Event ManagementDocument71 pagesIntroduction To Patient Safety Analysis and Event ManagementPaolo VegaNo ratings yet
- Philosophy of Education MSN-2Document37 pagesPhilosophy of Education MSN-2Paolo VegaNo ratings yet
- Introduction To ShockDocument56 pagesIntroduction To ShockPaolo VegaNo ratings yet
- Linking Hospital Managers To LiteratureDocument32 pagesLinking Hospital Managers To LiteraturePaolo VegaNo ratings yet
- Apply CuspDocument26 pagesApply CuspPaolo VegaNo ratings yet
- Beacon HandbookDocument30 pagesBeacon HandbookPaolo VegaNo ratings yet
- Ann Deerhake, MS, RN, CNL, CCRN: CNL USF Conference Logo 2011Document35 pagesAnn Deerhake, MS, RN, CNL, CCRN: CNL USF Conference Logo 2011Paolo VegaNo ratings yet
- Introduction To ShockDocument56 pagesIntroduction To ShockPaolo VegaNo ratings yet
- CCRN Review Part 1: "Never Let What You Cannot Do Interfere With What You Can Do"Document160 pagesCCRN Review Part 1: "Never Let What You Cannot Do Interfere With What You Can Do"Paolo VegaNo ratings yet
- Eb PN LectureDocument54 pagesEb PN LecturePaolo VegaNo ratings yet
- CCRNPart 2Document164 pagesCCRNPart 2Paolo Vega100% (5)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- FEU Review Pre Board Exam 2016 PathophysioDocument8 pagesFEU Review Pre Board Exam 2016 PathophysioDharlyn MungcalNo ratings yet
- Journal of Ayurveda and Integrative Medicine: Apar Avinash Saoji, B.R. Raghavendra, N.K. ManjunathDocument9 pagesJournal of Ayurveda and Integrative Medicine: Apar Avinash Saoji, B.R. Raghavendra, N.K. ManjunathALiint Nissa NisaniestNo ratings yet
- Acute Inferior Myocardial Infarction - ARTICLEDocument4 pagesAcute Inferior Myocardial Infarction - ARTICLEJonathan MorenoNo ratings yet
- Cardiac EnzymesDocument25 pagesCardiac EnzymesMonette Abalos MendovaNo ratings yet
- Brosur A4 Albunorm25 2021-FinalsDocument2 pagesBrosur A4 Albunorm25 2021-FinalsVerico PratamaNo ratings yet
- Prehospital Emergency Care 11th Edition 11th EditionDocument61 pagesPrehospital Emergency Care 11th Edition 11th Editionmarion.wade94398% (42)
- BIO - F5 - KSSM - CHAPTER - 1 - 1.1 and 1.2 ORGANISATION OF PLANT TISSUES AND GROWTHDocument59 pagesBIO - F5 - KSSM - CHAPTER - 1 - 1.1 and 1.2 ORGANISATION OF PLANT TISSUES AND GROWTHwienna1987100% (2)
- SOMNOcheck MicroDocument2 pagesSOMNOcheck MicroEvangelosNo ratings yet
- Introduction To Transfusion MedicineDocument12 pagesIntroduction To Transfusion MedicineSamantha BuiNo ratings yet
- MD-7 HearttDocument28 pagesMD-7 HearttvincenzoNo ratings yet
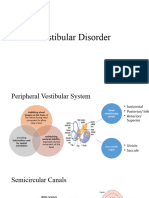
- Vestibular DisorderDocument22 pagesVestibular DisorderSumbal SalikNo ratings yet
- Fisio1 Exc6 Act1Document5 pagesFisio1 Exc6 Act1Fadli Nurul HanifNo ratings yet
- 14-11-22 Malam Dr. YolaDocument6 pages14-11-22 Malam Dr. YolabobynandaNo ratings yet
- Sicksinussyndrome: Roberto de Ponti,, Jacopo Marazzato,, Giuseppe Bagliani,, Fabio M. Leonelli,, Luigi PadelettiDocument13 pagesSicksinussyndrome: Roberto de Ponti,, Jacopo Marazzato,, Giuseppe Bagliani,, Fabio M. Leonelli,, Luigi Padelettijose noel garcia perezNo ratings yet
- ElectrolytesDocument2 pagesElectrolytestentenNo ratings yet
- 1st Prof Examination 2023Document12 pages1st Prof Examination 2023Masoom IgNo ratings yet
- Lesson 5 ECG BiopacDocument6 pagesLesson 5 ECG BiopacJavier VeintimillaNo ratings yet
- NC Fauzi ERIADocument21 pagesNC Fauzi ERIADodi DiNo ratings yet
- Chapter 2Document35 pagesChapter 2Amiey SehokNo ratings yet
- Slides AUTACOIDSDocument29 pagesSlides AUTACOIDSStrange eeNo ratings yet
- Notes On Coordination - Response - Nervous System, Reflex Arc, Type of NeuronesDocument6 pagesNotes On Coordination - Response - Nervous System, Reflex Arc, Type of NeuronesamberNo ratings yet
- Electrolyte Disorders: Camiron L. Pfennig Corey M. SlovisDocument19 pagesElectrolyte Disorders: Camiron L. Pfennig Corey M. SlovisMayra Itzel Guerrero ChavezNo ratings yet
- NURSING CARE PLAN Alvarez - Impaired Gas ExchangeDocument2 pagesNURSING CARE PLAN Alvarez - Impaired Gas ExchangeNader AbdurasadNo ratings yet
- Central and Peripheral Factors in FatigueDocument6 pagesCentral and Peripheral Factors in FatigueEduardo VieyraNo ratings yet
- Polymyolitis NCP 2Document1 pagePolymyolitis NCP 2Alexa Lexington Rae ZagadoNo ratings yet
- HeartDocument38 pagesHeartanuzNo ratings yet
- HOMEOSTASISDocument24 pagesHOMEOSTASISBasty BERNALESNo ratings yet
- Regional Circulation: Prof. K. SivapalanDocument23 pagesRegional Circulation: Prof. K. SivapalanjikookNo ratings yet
- Coronary Artery Disease Pathophysiology PDFDocument3 pagesCoronary Artery Disease Pathophysiology PDFMohd Amir Bin Bashir0% (1)
- MSN Exam For Increased Intracranial PressureDocument4 pagesMSN Exam For Increased Intracranial PressureLorelyn Santos CorpuzNo ratings yet