You might also like
- 2010 CHEP - RecommendationsDocument5 pages2010 CHEP - RecommendationsArdhito BudhijuwonoNo ratings yet
- 2007 Guidelines For The Management of Arterial European Heart AssossDocument75 pages2007 Guidelines For The Management of Arterial European Heart AssossYeniNo ratings yet
- Physical Examination of Cardiovascular: DR - Ira Andaningsih SPJP Cardiovascular Block 2008Document89 pagesPhysical Examination of Cardiovascular: DR - Ira Andaningsih SPJP Cardiovascular Block 2008YeniNo ratings yet
- The Overview of Hypertension 2009Document50 pagesThe Overview of Hypertension 2009YeniNo ratings yet
- Rational Drug Treatment2011Document27 pagesRational Drug Treatment2011YeniNo ratings yet
- History TakingDocument28 pagesHistory TakingYeniNo ratings yet
- Film Session Grey's AnatomyDocument4 pagesFilm Session Grey's AnatomyYeniNo ratings yet
- Metabolisme B-12 and FolateDocument9 pagesMetabolisme B-12 and FolateYeniNo ratings yet
- Print-Slide DR DinaDocument4 pagesPrint-Slide DR DinaYeniNo ratings yet
- Lo w1Document12 pagesLo w1YeniNo ratings yet
- Anemia UPHDocument24 pagesAnemia UPHYeniNo ratings yet
- Print-Slide DR DinaDocument4 pagesPrint-Slide DR DinaYeniNo ratings yet
- Appropriate Use of Tests For Folate and Vitamin B12 DeficiencyDocument4 pagesAppropriate Use of Tests For Folate and Vitamin B12 DeficiencyYeniNo ratings yet
- Anemia FarmakoDocument28 pagesAnemia FarmakoYeniNo ratings yet
- Erythrocyte Life Cycle: PathophysiologyDocument15 pagesErythrocyte Life Cycle: PathophysiologyYeniNo ratings yet
- Anemia, Rhesus and Blood Group Incompatibility inDocument42 pagesAnemia, Rhesus and Blood Group Incompatibility inYeniNo ratings yet
- Erythropoiesis and Bilirubin Metabolism: V. Sutarmo SetiadjiDocument16 pagesErythropoiesis and Bilirubin Metabolism: V. Sutarmo SetiadjiYeniNo ratings yet
- Anemia ClinskillDocument15 pagesAnemia ClinskillYeniNo ratings yet
- Syncope VonnyDocument41 pagesSyncope VonnyYeniNo ratings yet
- Syncope VonnyDocument41 pagesSyncope VonnyYeniNo ratings yet
- Dr. Haryanto - Kuliah Anemi Deff Fe 2011Document20 pagesDr. Haryanto - Kuliah Anemi Deff Fe 2011YeniNo ratings yet
- Plenary Lecture Multiple Trauma by FredaDocument19 pagesPlenary Lecture Multiple Trauma by FredaYeniNo ratings yet
- Clinical Approach to AnemiaDocument23 pagesClinical Approach to AnemiaYeniNo ratings yet
- Nosocomial Infection UphDocument77 pagesNosocomial Infection UphYeniNo ratings yet
- Nosocomial Infection UphDocument77 pagesNosocomial Infection UphYeniNo ratings yet
- Head InjuryDocument40 pagesHead InjuryYeniNo ratings yet
- Week 4 - Fungi Effector Mechanism of IRDocument67 pagesWeek 4 - Fungi Effector Mechanism of IRYeniNo ratings yet
- Anti VirusDocument36 pagesAnti VirusYeniNo ratings yet
- Tabel AntibiotikDocument5 pagesTabel AntibiotikYeniNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- NTP To IRIG-B DatasheetDocument1 pageNTP To IRIG-B Datasheetrpaliwal1967No ratings yet
- CM 3Document96 pagesCM 3Janak Bahadur RokayaNo ratings yet
- 01.introduction To Earth ScienceDocument29 pages01.introduction To Earth ScienceIshan Chua100% (1)
- College Students' Homesickness: An Interpretative PhenomenologyDocument9 pagesCollege Students' Homesickness: An Interpretative PhenomenologyGodfrey CasinilloNo ratings yet
- DLL 10-11Document5 pagesDLL 10-11LORIBELLE MALDEPENANo ratings yet
- RFP-phase-VI - 27 05 2020Document100 pagesRFP-phase-VI - 27 05 2020Jagdish JoshiNo ratings yet
- Uws Threat Hunting 101 White Paper PDFDocument25 pagesUws Threat Hunting 101 White Paper PDFJacob StamperNo ratings yet
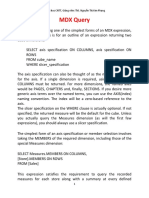
- Introduction To MDX - KPDocument10 pagesIntroduction To MDX - KPTiến Hồ MạnhNo ratings yet
- Maintenance ManualDocument14 pagesMaintenance ManualAdrian Lau100% (1)
- Filtered Battery Charger / DC Power Supply: Installation & Operation ManualDocument50 pagesFiltered Battery Charger / DC Power Supply: Installation & Operation ManualQazi M Asim WasimNo ratings yet
- What Is Organizational Design - Types and ExamplesDocument7 pagesWhat Is Organizational Design - Types and ExamplesSubradip debnathNo ratings yet
- Pantoprazole Tablets USP-32Document7 pagesPantoprazole Tablets USP-32Nikhil SindhavNo ratings yet
- Post-Earthquake Report On Bamboo Structures and Recommendations For Reconstruction With Bamboo On The Ecuadorian CoastDocument36 pagesPost-Earthquake Report On Bamboo Structures and Recommendations For Reconstruction With Bamboo On The Ecuadorian CoastRUENo ratings yet
- Tromet 092013 Rep PDFDocument19 pagesTromet 092013 Rep PDFErik SnchzNo ratings yet
- Nursing Research Chapter3Document4 pagesNursing Research Chapter3Sj Cams100% (2)
- Reflection of Physical EducationDocument6 pagesReflection of Physical Educationapi-235007312No ratings yet
- The OZ Principle - InsightsDocument24 pagesThe OZ Principle - InsightsJesus Camacho100% (3)
- Body Defence MechanismsDocument11 pagesBody Defence MechanismsJoyce TaiNo ratings yet
- Kinder Q2 - Week 10 For CO Lesson PlanDocument4 pagesKinder Q2 - Week 10 For CO Lesson PlanCleofe Joy Juan Magturo100% (2)
- 41Cr4 Chemical PDFDocument2 pages41Cr4 Chemical PDFGayathriRajasekaranNo ratings yet
- HMT Ass 1Document2 pagesHMT Ass 1Sachin PalNo ratings yet
- Jurnal Self CareDocument7 pagesJurnal Self CareIkhe MakaghanaNo ratings yet
- Aol Act 11 RandyDocument3 pagesAol Act 11 RandyaksanaNo ratings yet
- Thermodynamic processes and energy transfers in open and closed systemsDocument12 pagesThermodynamic processes and energy transfers in open and closed systemsravitejabvNo ratings yet
- Ultimate List of ISO Standards For Medical Devices-1Document34 pagesUltimate List of ISO Standards For Medical Devices-1Sridharan PadmanabhanNo ratings yet
- GA ClassificationDocument32 pagesGA ClassificationFernando GómezNo ratings yet
- The Breath of LifeDocument6 pagesThe Breath of Lifekabshiel100% (1)
- Psa 700 Notes and SummaryDocument10 pagesPsa 700 Notes and SummaryEjkNo ratings yet
- Asad Durrani - Pakistan Adrift - Navigating Troubled Waters-Hurst, Oxford University Press (2018)Document263 pagesAsad Durrani - Pakistan Adrift - Navigating Troubled Waters-Hurst, Oxford University Press (2018)Junaid AliNo ratings yet
- HuDocument13 pagesHujt626No ratings yet