You might also like
- Glargine and CancerDocument13 pagesGlargine and Cancerfarmasi_hmNo ratings yet
- Major Depressive DisordersDocument22 pagesMajor Depressive Disordersfarmasi_hm100% (2)
- Food ContaminationDocument19 pagesFood Contaminationfarmasi_hm100% (2)
- New & Emerging Treatment of Diabetic Retinopathy: Presented By: Pauline Teo Siew Chin 7th January, 2009Document42 pagesNew & Emerging Treatment of Diabetic Retinopathy: Presented By: Pauline Teo Siew Chin 7th January, 2009farmasi_hmNo ratings yet
- Diabetic KetoacidosisDocument12 pagesDiabetic Ketoacidosisfarmasi_hmNo ratings yet
- AcneDocument24 pagesAcnefarmasi_hm100% (2)
- Deep Vein Thrombosis - 2003Document34 pagesDeep Vein Thrombosis - 2003farmasi_hm100% (1)
- Head LiceDocument15 pagesHead Licefarmasi_hmNo ratings yet
- Emergency ContraceptionDocument24 pagesEmergency Contraceptionfarmasi_hm100% (1)
- Peptic Ulcer DiseaseDocument26 pagesPeptic Ulcer Diseasefarmasi_hmNo ratings yet
- Atopic Dermatitis (Eczema)Document19 pagesAtopic Dermatitis (Eczema)farmasi_hmNo ratings yet
- Medication Safety UnitDocument58 pagesMedication Safety Unitfarmasi_hmNo ratings yet
- Management of Septic Shock in AdultsDocument28 pagesManagement of Septic Shock in Adultsfarmasi_hmNo ratings yet
- Atrial Fibrillation (AF)Document24 pagesAtrial Fibrillation (AF)farmasi_hm100% (1)
- Syndrome of Inappropriate Secretion of Anti Diuretic HormoneDocument39 pagesSyndrome of Inappropriate Secretion of Anti Diuretic Hormonefarmasi_hmNo ratings yet
- Diuretics: Sumolly Anak DavidDocument29 pagesDiuretics: Sumolly Anak Davidfarmasi_hmNo ratings yet
- WarfarinDocument21 pagesWarfarinfarmasi_hmNo ratings yet
- ADR Reporting, Medication Error Reporting SystemDocument100 pagesADR Reporting, Medication Error Reporting Systemfarmasi_hm100% (1)
- Sinusitis & Its TreatmentDocument20 pagesSinusitis & Its Treatmentfarmasi_hmNo ratings yet
- HPV Infection StephDocument25 pagesHPV Infection Stephfarmasi_hmNo ratings yet
- Leptospirosis: Pauline Teo Siew ChinDocument18 pagesLeptospirosis: Pauline Teo Siew Chinfarmasi_hmNo ratings yet
- Angiotensin Receptor Blockers (O)Document26 pagesAngiotensin Receptor Blockers (O)farmasi_hmNo ratings yet
- Otc Treatment For Muscle Sprain & StrainsDocument12 pagesOtc Treatment For Muscle Sprain & Strainsfarmasi_hmNo ratings yet
- Overview of Nephrotic SyndromeDocument19 pagesOverview of Nephrotic Syndromefarmasi_hm100% (1)
- Over-The-Counter Foot CareDocument17 pagesOver-The-Counter Foot Carefarmasi_hmNo ratings yet
- Calcium Channel BlockersDocument15 pagesCalcium Channel Blockersfarmasi_hm100% (2)
- Hyperemesis Gravidarum: Causes, Symptoms and TreatmentDocument13 pagesHyperemesis Gravidarum: Causes, Symptoms and TreatmentBang JuntakNo ratings yet
- IntroductionDocument21 pagesIntroductionfarmasi_hmNo ratings yet
- OTC PregnancyDocument11 pagesOTC Pregnancyfarmasi_hmNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
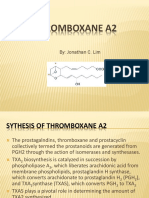
- Thromboxane A2Document16 pagesThromboxane A2Concepcion R. Aquino0% (1)
- Cape Biology 2014 U2 p1Document12 pagesCape Biology 2014 U2 p1FiveLimaRomeo100% (4)
- A Survey On The Awareness of PneumoniaDocument2 pagesA Survey On The Awareness of PneumoniaAshy LeeNo ratings yet
- AAO 2015 Instruction Course (Mystery Retina-Interactive Discussion of Cases) - Final HandoutDocument45 pagesAAO 2015 Instruction Course (Mystery Retina-Interactive Discussion of Cases) - Final HandoutJennifer Kang-MielerNo ratings yet
- Stevens (Science) Med TechDocument31 pagesStevens (Science) Med TechnotsoninjaninjaNo ratings yet
- IAS Mains Zoology 2016Document8 pagesIAS Mains Zoology 2016Rehaan FayazNo ratings yet
- MAT2379 Practice MidtermDocument9 pagesMAT2379 Practice MidtermAshNo ratings yet
- Fundamental Techniques in Cell Culture 3rd EditionDocument84 pagesFundamental Techniques in Cell Culture 3rd EditionCM Najito100% (1)
- Fibrous Dysplasia of BoneDocument31 pagesFibrous Dysplasia of Bonet.babyNo ratings yet
- مختبر مايكرو 2و 3 و 4 PDFDocument13 pagesمختبر مايكرو 2و 3 و 4 PDFAhmed Assaf100% (1)
- Grammar Test (04-21)Document4 pagesGrammar Test (04-21)Clarence De LeonNo ratings yet
- Exposure To Ambient Fine Particles Causes Abnormal Energy Metabolism and ATP Decrease in Lung TissuesDocument10 pagesExposure To Ambient Fine Particles Causes Abnormal Energy Metabolism and ATP Decrease in Lung TissuesMaria Elena Gonzalez DiazNo ratings yet
- 9 Exercise Physiology Handout 2011Document20 pages9 Exercise Physiology Handout 2011maraj687No ratings yet
- Identification of Pseudomonas SPDocument20 pagesIdentification of Pseudomonas SPUttam Kr Patra100% (4)
- Do I Have Chronic Fatigue SyndromeDocument10 pagesDo I Have Chronic Fatigue SyndromecassseaNo ratings yet
- (ASM Books) Jane Flint, Vincent R. Racaniello, Glenn F. Rall, Theodora Hatziioannou, Anna Marie Skalka - Principles of Virology-ASM Press (2020)Document1,131 pages(ASM Books) Jane Flint, Vincent R. Racaniello, Glenn F. Rall, Theodora Hatziioannou, Anna Marie Skalka - Principles of Virology-ASM Press (2020)Ming YanNo ratings yet
- Melkersson Rosenthal SyndromeDocument3 pagesMelkersson Rosenthal SyndromeKartikakhairaniNo ratings yet
- Mineralocorticoids: Shajeer. SDocument42 pagesMineralocorticoids: Shajeer. SShajeer SalimNo ratings yet
- Cell DivisionDocument43 pagesCell Divisionjanahf0% (1)
- 500 SBA Gen SystemicDocument27 pages500 SBA Gen Systemicdr_shafiqNo ratings yet
- AbortionDocument42 pagesAbortionKondapavuluru Jyothi50% (2)
- GMO - Friend or Foe?Document17 pagesGMO - Friend or Foe?jpfarreNo ratings yet
- Nbme Cbse Actual Test Questions and AnswersDocument175 pagesNbme Cbse Actual Test Questions and Answersgithijidennis99No ratings yet
- Biology Definitions by Vasumitra GajbhiyeDocument3 pagesBiology Definitions by Vasumitra GajbhiyeHuzaifa ImranNo ratings yet
- Cardiac+Electrophysiology +From+Cell+to+BesideDocument1,113 pagesCardiac+Electrophysiology +From+Cell+to+BesideduyquanNo ratings yet
- Glomerular Diseases: Assistant Professor Dr. Shumaila Rafi MedicineDocument17 pagesGlomerular Diseases: Assistant Professor Dr. Shumaila Rafi MedicineMuhammad MakkiNo ratings yet
- Hygiena Product Catalog 2018 WebDocument92 pagesHygiena Product Catalog 2018 WebLuthfi Nur AlwiNo ratings yet
- Stickler Syndrome and HomoeopathyDocument9 pagesStickler Syndrome and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Epidemiology of Communicable DiseasesDocument3 pagesEpidemiology of Communicable Diseasessarguss14100% (4)
- Silicon risk assessment summaryDocument7 pagesSilicon risk assessment summaryYoami PerdomoNo ratings yet