You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Respiration One 2Document70 pagesRespiration One 2api-19916399100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Blood CoagulationDocument70 pagesBlood Coagulationapi-19916399No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- XIII EndocrinologyDocument87 pagesXIII Endocrinologyapi-19916399100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Respiration TwoDocument58 pagesRespiration Twoapi-19916399No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Respiration 3Document23 pagesRespiration 3api-19916399100% (1)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Respiration TwoDocument58 pagesRespiration Twoapi-19916399No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Respiration OneDocument75 pagesRespiration Oneapi-19916399No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Physiology of Blood VesselDocument65 pagesPhysiology of Blood Vesselapi-19916399No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Neurophysiology: Run Fight Speak Think Watch Listen Taste SmellDocument22 pagesNeurophysiology: Run Fight Speak Think Watch Listen Taste Smellapi-19916399No ratings yet
- Preload and AfterloadDocument28 pagesPreload and Afterloadapi-19916399100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Physiology Answers and ExDocument19 pagesPhysiology Answers and Exapi-19916399No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Physiology - Retired QuestionsDocument12 pagesPhysiology - Retired Questionsapi-19916399No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Regulation of Systemic Arterial PressureDocument29 pagesRegulation of Systemic Arterial Pressureapi-19916399No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Physiology Answers and ExDocument19 pagesPhysiology Answers and Exapi-19916399No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Physiology - Retired QuestionsDocument12 pagesPhysiology - Retired Questionsapi-19916399No ratings yet
- Nervous System 6Document27 pagesNervous System 6api-19916399No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Nervous System 7Document20 pagesNervous System 7api-19916399No ratings yet
- Nervous System 3Document29 pagesNervous System 3api-19916399No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Jingying T.A. Department of PhysiologyDocument19 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- 01.introduction To PhysiologyDocument44 pages01.introduction To Physiologyapi-19916399No ratings yet
- Jingying T.A. Department of PhysiologyDocument22 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Jingying T.A. Department of PhysiologyDocument26 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- KidneyDocument203 pagesKidneyapi-19916399100% (1)
- Electrical Activity of The HeartDocument29 pagesElectrical Activity of The Heartapi-19916399No ratings yet
- Electrophysiological Properties of Cardiac MyocytesDocument39 pagesElectrophysiological Properties of Cardiac Myocytesapi-19916399No ratings yet
- Gastrointestinal PhysiologyDocument134 pagesGastrointestinal Physiologyapi-19916399100% (1)
- Heart Valve DiseaseDocument43 pagesHeart Valve Diseaseapi-19916399100% (1)
- Gastrointestinal PhysiologDocument133 pagesGastrointestinal Physiologapi-19916399100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Evaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac IndexDocument53 pagesEvaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac Indexapi-19916399No ratings yet
- Kyuhyun Wang, MD: What Is The Rhythm?Document43 pagesKyuhyun Wang, MD: What Is The Rhythm?api-19916399No ratings yet
- INTUSSUSCEPTIONDocument3 pagesINTUSSUSCEPTIONS GNo ratings yet
- Billiary SystemDocument60 pagesBilliary SystemDONALD UNASHENo ratings yet
- Crohns DiseaseDocument32 pagesCrohns DiseaseMin Chi PakNo ratings yet
- Daftar Pustaka - 4Document3 pagesDaftar Pustaka - 4PascaIKM STIKes KuninganNo ratings yet
- Esophagitis: SymptomsDocument4 pagesEsophagitis: SymptomsRoyster CabralNo ratings yet
- Gastroenterology - DiverticulaDocument1 pageGastroenterology - DiverticulaEugen MNo ratings yet
- UTS Daring 2021Document32 pagesUTS Daring 2021Akdri Bagus ZulvikarNo ratings yet
- Gastro Review QuestionsDocument9 pagesGastro Review QuestionsPortia Dulce Patatag ToqueroNo ratings yet
- GastroenterologyDocument30 pagesGastroenterologyMohammad MohyeddienNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Peptic UlcerDocument59 pagesPeptic UlcerfloramaeyecyecNo ratings yet
- Presented By:: Alia - Farooq & Zahra - AbbasDocument43 pagesPresented By:: Alia - Farooq & Zahra - AbbasZahra MotorwalaNo ratings yet
- My Notes For USMLEDocument48 pagesMy Notes For USMLEaesfafafaNo ratings yet
- LaxativesDocument1 pageLaxativesapi-3739910No ratings yet
- Abdominal Pain - Royal Children HospitalDocument4 pagesAbdominal Pain - Royal Children HospitalMehrdad IraniNo ratings yet
- TextDocument17 pagesTextnaser zoabiNo ratings yet
- PT Asuransi Jiwa Inhealth IndonesiaDocument1 pagePT Asuransi Jiwa Inhealth Indonesiabob saragihNo ratings yet
- Acute AbdomenDocument31 pagesAcute AbdomenWildan AngelouNo ratings yet
- Anal Fissures & FistulasDocument3 pagesAnal Fissures & FistulasLouis FortunatoNo ratings yet
- DiverticularDocument2 pagesDiverticularnimishgpatelNo ratings yet
- Fissure Treatment in MumbaiDocument4 pagesFissure Treatment in MumbaiSambit ClinicNo ratings yet
- 10 Foods To Avoid For Diverticulitis Diet - 10FAQDocument5 pages10 Foods To Avoid For Diverticulitis Diet - 10FAQRay ManzanillaNo ratings yet
- Hubungan Usia Dengan EmesisDocument7 pagesHubungan Usia Dengan EmesisNahar RuddinNo ratings yet
- DS - Senokot ForteDocument1 pageDS - Senokot ForteMarjorie Dela RosaNo ratings yet
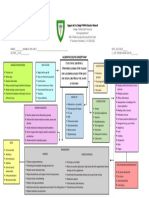
- Ulcerative Colitis Concept MapDocument1 pageUlcerative Colitis Concept MapIris MambuayNo ratings yet
- Lower Gi Case Presentation PDFDocument35 pagesLower Gi Case Presentation PDFapi-448999672No ratings yet
- DR Kiki Lukman Patofisiologi Acute CholangitisDocument36 pagesDR Kiki Lukman Patofisiologi Acute CholangitisAfkar30No ratings yet
- Plabable-Gems-6. Gastroenterology Plabable GemsDocument39 pagesPlabable-Gems-6. Gastroenterology Plabable GemsHabo Habo100% (1)
- Case StudyDocument18 pagesCase StudyNovaWulandariPalufiNo ratings yet
- Peptic Ulcer LPDocument8 pagesPeptic Ulcer LPAnonymous 0C4OZmR100% (2)
- Assess BowelDocument2 pagesAssess BowelneoclintNo ratings yet