You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Closing The Cancer Divide & Strengthening Health Systems: Interwoven OpportunitiesDocument39 pagesClosing The Cancer Divide & Strengthening Health Systems: Interwoven OpportunitiesPresentaciones_FKNo ratings yet
- Innovations in Breast Cancer TreatmentDocument21 pagesInnovations in Breast Cancer TreatmentPresentaciones_FKNo ratings yet
- Closing The Global Pain Divide: An Equity and Health ImperativeDocument16 pagesClosing The Global Pain Divide: An Equity and Health ImperativePresentaciones_FKNo ratings yet
- The Health and Caregiving Workforce: An Array of InequitiesDocument16 pagesThe Health and Caregiving Workforce: An Array of InequitiesPresentaciones_FKNo ratings yet
- Unpaid Health Care and Caregiving: A Gendered and Hidden Yet Indispensable Subsidy To Economic and Social Development.Document16 pagesUnpaid Health Care and Caregiving: A Gendered and Hidden Yet Indispensable Subsidy To Economic and Social Development.Presentaciones_FKNo ratings yet
- Closing Cancer Divided: Expanding Access To Care & ControlDocument46 pagesClosing Cancer Divided: Expanding Access To Care & ControlPresentaciones_FKNo ratings yet
- La Mujer Ante El COVID-19: Retos y Oportunidades para La Salud y El Sector Salud.Document36 pagesLa Mujer Ante El COVID-19: Retos y Oportunidades para La Salud y El Sector Salud.Presentaciones_FKNo ratings yet
- Closing The Cancer DivideDocument36 pagesClosing The Cancer DividePresentaciones_FKNo ratings yet
- Health System Responses To Women's Cancers in The AmericasDocument36 pagesHealth System Responses To Women's Cancers in The AmericasPresentaciones_FKNo ratings yet
- Closing The Divide in Access To Palliative Care and Pain ReliefDocument45 pagesClosing The Divide in Access To Palliative Care and Pain ReliefPresentaciones_FKNo ratings yet
- Breast Cancer in The Americas: Closing Divides Through Systemic Innovation & AdvocacyDocument33 pagesBreast Cancer in The Americas: Closing Divides Through Systemic Innovation & AdvocacyPresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief.Document37 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief.Presentaciones_FKNo ratings yet
- Breast Cancer Disparities: Closing Global DividesDocument37 pagesBreast Cancer Disparities: Closing Global DividesPresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief: An Imperative of Universal Health CoverageDocument36 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief: An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Breast Cancer in The AmericasDocument27 pagesBreast Cancer in The AmericasPresentaciones_FKNo ratings yet
- Closing Cancer Divided: Expanding Access To Care & ControlDocument41 pagesClosing Cancer Divided: Expanding Access To Care & ControlPresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument19 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Closing The Cancer Divide: Lessons From Women's HealthDocument43 pagesClosing The Cancer Divide: Lessons From Women's HealthPresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument44 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Closing Divides To Meet The Challenge of Women S CancerDocument22 pagesClosing Divides To Meet The Challenge of Women S CancerPresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument16 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Closing The Cancer Divide For Women in The Americas: Diagonal Health System InnovationsDocument39 pagesClosing The Cancer Divide For Women in The Americas: Diagonal Health System InnovationsPresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument18 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Reducing The Cancer Divide For Breast and Cervical CancerDocument53 pagesReducing The Cancer Divide For Breast and Cervical CancerPresentaciones_FKNo ratings yet
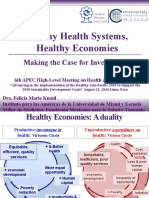
- Healthy Health Systems, Healthy Economies. Making The Case For Investment.Document28 pagesHealthy Health Systems, Healthy Economies. Making The Case For Investment.Presentaciones_FKNo ratings yet
- Evidence-Inspired Advocacy and Advocacy-Based EvidenceDocument35 pagesEvidence-Inspired Advocacy and Advocacy-Based EvidencePresentaciones_FKNo ratings yet
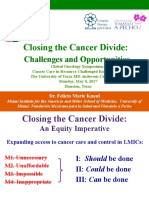
- Closing The Cancer Divide: Challenges and OpportunitiesDocument51 pagesClosing The Cancer Divide: Challenges and OpportunitiesPresentaciones_FKNo ratings yet
- Evidence-Inspired Advocacy and Advocacy-Based EvidenceDocument35 pagesEvidence-Inspired Advocacy and Advocacy-Based EvidencePresentaciones_FKNo ratings yet
- Women's Cancers in The Americas: Closing DividesDocument35 pagesWomen's Cancers in The Americas: Closing DividesPresentaciones_FKNo ratings yet
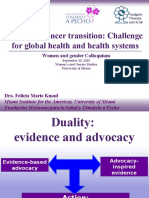
- Women's Cancer Transition: Challenge For Global Health and Health SystemsDocument58 pagesWomen's Cancer Transition: Challenge For Global Health and Health SystemsPresentaciones_FKNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DOH ICT SytemDocument19 pagesDOH ICT Sytemricohizon99No ratings yet
- Pharmaceutical Issues When Crushing, Opening or Splitting Oral Dosage FormsDocument7 pagesPharmaceutical Issues When Crushing, Opening or Splitting Oral Dosage FormsMohamed OmerNo ratings yet
- RCOG Recomendation For Treating HEGDocument27 pagesRCOG Recomendation For Treating HEGleliamediaNo ratings yet
- Standard Operating Procedures in Pharmaceutical IndustryDocument38 pagesStandard Operating Procedures in Pharmaceutical IndustryDevavrat Singh25% (4)
- Good Medicine by Patrick Holford: IntroductionDocument12 pagesGood Medicine by Patrick Holford: IntroductionLittle Brown UK100% (4)
- Class 12 Polymer Chemistry and Chemistry in Everyday LifeDocument9 pagesClass 12 Polymer Chemistry and Chemistry in Everyday LifeMeghna AshokNo ratings yet
- New Prescription For Drug Makers - Update The Plants - WSJDocument5 pagesNew Prescription For Drug Makers - Update The Plants - WSJStacy Kelly100% (1)
- Teva Pharmaceutical Industries Limited (TEVA) - Pharmaceuticals & Healthcare - Deals and Alliances ProfileDocument342 pagesTeva Pharmaceutical Industries Limited (TEVA) - Pharmaceuticals & Healthcare - Deals and Alliances ProfileJyoti KhatriNo ratings yet
- SPLDocument116 pagesSPLNikhil KhobragadeNo ratings yet
- Competition PharmaceuticalsDocument47 pagesCompetition Pharmaceuticalsavp24No ratings yet
- Overview of Pharmaceutical ManufacturingDocument14 pagesOverview of Pharmaceutical ManufacturingFauz ShereNo ratings yet
- Benharm 2Document7 pagesBenharm 2Hurriya Nur AldillaNo ratings yet
- Integrity of The Pharmaceutical Supply Chain:: Product Sourcing For Patient SafetyDocument10 pagesIntegrity of The Pharmaceutical Supply Chain:: Product Sourcing For Patient SafetymurugananthCNo ratings yet
- 1.pharmacy Technician Study GuideDocument31 pages1.pharmacy Technician Study GuideAlan Hao92% (12)
- Community Pharmacy Practice in PakistanDocument18 pagesCommunity Pharmacy Practice in Pakistanthundercat123No ratings yet
- The Indian Pharma Industry PDFDocument24 pagesThe Indian Pharma Industry PDFSnehith AlapatiNo ratings yet
- DepressionDocument18 pagesDepressionapi-238280299No ratings yet
- Price List of BooksDocument32 pagesPrice List of BooksUtc ChattanoogaNo ratings yet
- Adroit, Ehospital ProposalDocument14 pagesAdroit, Ehospital Proposalkamalendusingh1No ratings yet
- Quality Specifications enDocument42 pagesQuality Specifications enkhaoula attiaNo ratings yet
- Treatment of Psychiatric Disorders in CKDDocument13 pagesTreatment of Psychiatric Disorders in CKDmplennaNo ratings yet
- Alternative Health & Herbs Remedies 425 Jackson SE, Albany, OR 97321 1-541-791-8400Document159 pagesAlternative Health & Herbs Remedies 425 Jackson SE, Albany, OR 97321 1-541-791-8400Marvin T Verna100% (2)
- Descriptive Study On The Common Violations Committed in The Issuance of Prescription FormsDocument54 pagesDescriptive Study On The Common Violations Committed in The Issuance of Prescription FormskasamahumanrightsNo ratings yet
- A Woman's Guide To HerbsDocument15 pagesA Woman's Guide To Herbsfiz1432100% (1)
- Nurse-Patient Trust RelationshipDocument12 pagesNurse-Patient Trust RelationshipMarina Costa100% (1)
- Microeconomics Pharmaceutical IndustryDocument4 pagesMicroeconomics Pharmaceutical Industryapi-242801321No ratings yet
- MTM ModuleDocument45 pagesMTM ModuleChang CaiNo ratings yet
- Trainig and DevelopmentDocument120 pagesTrainig and Developmentaccord123100% (1)
- (INTERN 1) Exercise 2Document2 pages(INTERN 1) Exercise 2Sebastian MoronNo ratings yet