You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Drug Nomenclature HintsDocument1 pageDrug Nomenclature HintsJordynNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Medication Dosage and CalculationsDocument32 pagesMedication Dosage and CalculationsGavinTLDNo ratings yet
- Chapter 4 Practice TestDocument6 pagesChapter 4 Practice Testnursingstudentd100% (1)
- What Is 21 CFR Part 11Document26 pagesWhat Is 21 CFR Part 11chemtabNo ratings yet
- Pharmacology Study GuideDocument61 pagesPharmacology Study Guide32bballgoNo ratings yet
- A Sandpiper To Bring You JoyDocument3 pagesA Sandpiper To Bring You JoyShafira VidiastriNo ratings yet
- Happy IedDocument2 pagesHappy IedShafira VidiastriNo ratings yet
- Who Packs Your ParachuteDocument1 pageWho Packs Your ParachuteShafira VidiastriNo ratings yet
- Journal of Young InvestigatorsDocument3 pagesJournal of Young InvestigatorsShafira VidiastriNo ratings yet
- The 100 Most Beautiful Words in EnglishDocument5 pagesThe 100 Most Beautiful Words in EnglishShafira VidiastriNo ratings yet
- You Are Loved - A Story of FriendshipDocument3 pagesYou Are Loved - A Story of FriendshipShafira VidiastriNo ratings yet
- Types of ListeningDocument2 pagesTypes of ListeningShafira Vidiastri100% (1)
- Happy IedDocument2 pagesHappy IedShafira VidiastriNo ratings yet
- Yaris LeafletDocument2 pagesYaris Leafletnatta_anggoroNo ratings yet
- 5 Steps To Be Empathic ListenerDocument1 page5 Steps To Be Empathic ListenerShafira VidiastriNo ratings yet
- Starch1500 BrouchureDocument2 pagesStarch1500 BrouchureHeristiana PratiwiNo ratings yet
- 2023 NJ FormularyDocument104 pages2023 NJ FormularyPrince LiNo ratings yet
- Activity 7 Calculations Involved in Parenteral Therapy: University of Santo TomasDocument3 pagesActivity 7 Calculations Involved in Parenteral Therapy: University of Santo TomasJANNIE BELLE RODRIGUEZ100% (1)
- 2019-01 Introduction To Pharmaceutical EngineeringDocument7 pages2019-01 Introduction To Pharmaceutical EngineeringAndy HermanNo ratings yet
- ALL in 1Document1 pageALL in 1Shawn Gaurav JhaNo ratings yet
- 1 - State GMP 1Document52 pages1 - State GMP 1biocoalNo ratings yet
- Item Test Results Method Instrument: PKT 1 OF 6 - Lab Report-Released - (90385) PDFDocument2 pagesItem Test Results Method Instrument: PKT 1 OF 6 - Lab Report-Released - (90385) PDFinforumdocsNo ratings yet
- List Obat Salinan SalinanDocument3 pagesList Obat Salinan SalinanShishil LyaNo ratings yet
- Data Lemari Obat FixDocument7 pagesData Lemari Obat FixNuroniah Nuri LestariNo ratings yet
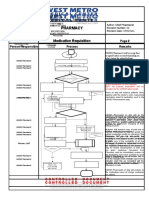
- Pharmacy Pharmacy: Medication Requisition Medication RequisitionDocument1 pagePharmacy Pharmacy: Medication Requisition Medication RequisitionSharie Grace ImlanNo ratings yet
- CTD Question and AnswersDocument17 pagesCTD Question and AnswersPraveenaNo ratings yet
- Dietary Effects On Drug Metabolism and Transport: Robert Z. Harris, Graham R. JangDocument18 pagesDietary Effects On Drug Metabolism and Transport: Robert Z. Harris, Graham R. JangFarah Fadhilah RamadhaniNo ratings yet
- Obat TemepelDocument7 pagesObat Temepelpuskesmas KalitiduNo ratings yet
- Smt. B.N.B Swaminarayan Pharmacy College, Salvav Dr. Kantilal Narkhede BP103TP Pharmaceutics 1 Question BankDocument6 pagesSmt. B.N.B Swaminarayan Pharmacy College, Salvav Dr. Kantilal Narkhede BP103TP Pharmaceutics 1 Question BankAvinash MansukNo ratings yet
- Drugs Approving AuthoritiesDocument38 pagesDrugs Approving AuthoritiesTariq HaqueNo ratings yet
- Pharmacology - PDFDocument41 pagesPharmacology - PDFTanaka KobayashiNo ratings yet
- Waktu Tunggu Pelayanan Resep Bpjs Rawat Jalan Di Instalasi Farmasi Rsia Anugrah Medical Center MetroDocument8 pagesWaktu Tunggu Pelayanan Resep Bpjs Rawat Jalan Di Instalasi Farmasi Rsia Anugrah Medical Center MetrohermaNo ratings yet
- ChloramphenicolDocument17 pagesChloramphenicolApurba Sarker Apu100% (1)
- Biosans LifecareDocument17 pagesBiosans LifecareLORD'S E PHARMACYNo ratings yet
- Medicine Update 2021 Section 14Document56 pagesMedicine Update 2021 Section 14Huda AminNo ratings yet
- Tingkat Signifikansi Kejadian Efek Samping Obat Berdasarkan Skala NaranjoDocument2 pagesTingkat Signifikansi Kejadian Efek Samping Obat Berdasarkan Skala Naranjolab pkmsekolaqNo ratings yet
- Worksheet 8Document2 pagesWorksheet 8Jocel OclaritNo ratings yet
- Vera Internship ReportDocument26 pagesVera Internship ReportLoïc steve Nyamsi BefouraNo ratings yet
- Prodrug Strategy: Concept & Applications)Document45 pagesProdrug Strategy: Concept & Applications)Nuwaira BalochNo ratings yet
- Cadd Question Bank 8 SemDocument8 pagesCadd Question Bank 8 SemMohammed KhalidNo ratings yet