You might also like
- NSTEMI GuideDocument33 pagesNSTEMI GuidefauziahNo ratings yet
- Arnold-Chiari Malformations Clinicl Features PDFDocument3 pagesArnold-Chiari Malformations Clinicl Features PDFsridharNo ratings yet
- LA Myxoma Case PresentationDocument34 pagesLA Myxoma Case PresentationWiwik Puji LestariNo ratings yet
- Right Ventricular Myocardial InfarctionDocument43 pagesRight Ventricular Myocardial Infarctionrudresh m g0% (2)
- Reye's SyndromeDocument11 pagesReye's SyndromeChristine Go100% (1)
- UrosepsisDocument22 pagesUrosepsisWita Ferani KartikaNo ratings yet
- Acute Coronary Syndrome: Dr. H.M. Saifullah Napu, SPJP, FihaDocument47 pagesAcute Coronary Syndrome: Dr. H.M. Saifullah Napu, SPJP, FihaJual Beli Promosi100% (1)
- 06prof. Riwanto-Abdominal Compartment SyndromeDocument41 pages06prof. Riwanto-Abdominal Compartment SyndromeTanujaa Venugopal100% (1)
- Fever of Unknown OriginDocument26 pagesFever of Unknown OriginFiona Yona Sitali100% (1)
- Angelina Alphonce JohoDocument80 pagesAngelina Alphonce JohoMerlina WijayawatiNo ratings yet
- Myocardial Infarction With ST Segment ElevationDocument27 pagesMyocardial Infarction With ST Segment ElevationRika Yulizah GobelNo ratings yet
- Congestive Heart FailureDocument19 pagesCongestive Heart FailureIlavenil PanduranganNo ratings yet
- Laporan Kasus Kardio CHF Ec CADDocument35 pagesLaporan Kasus Kardio CHF Ec CADpun212No ratings yet
- Cme Acs 2. Stemi (Izzah)Document36 pagesCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiNo ratings yet
- Acute Abdominal Pain in Children: Causes, Symptoms, DiagnosisDocument24 pagesAcute Abdominal Pain in Children: Causes, Symptoms, Diagnosisabdalmajeed alshammaryNo ratings yet
- Total Abdominal HysterectomyDocument19 pagesTotal Abdominal HysterectomyMeidina Rachma Amanda100% (1)
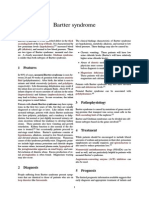
- Bartter Syndrome: Rare Inherited Kidney DisorderDocument3 pagesBartter Syndrome: Rare Inherited Kidney DisorderEnny Andriani100% (1)
- CCS 2019 STEMI GuidelinesDocument26 pagesCCS 2019 STEMI GuidelinesGazettNo ratings yet
- Agis Mira Dewi, S.kedDocument35 pagesAgis Mira Dewi, S.kedAgiish EMdeNo ratings yet
- Anaphylaxis Reaction & Drug Allergy 2Document47 pagesAnaphylaxis Reaction & Drug Allergy 2telusurNo ratings yet
- Trigeminal Neuralgia: Defination: According To Iasp (International Association For The Study of Pain)Document11 pagesTrigeminal Neuralgia: Defination: According To Iasp (International Association For The Study of Pain)saketaggarwalNo ratings yet
- Massive Ventral Hernia Case StudyDocument7 pagesMassive Ventral Hernia Case StudysugisweNo ratings yet
- IM AdconDocument28 pagesIM AdconCla SantosNo ratings yet
- Case Study: Congestive Heart FailureDocument7 pagesCase Study: Congestive Heart FailureXI-E / 21 / MARY TRIANANo ratings yet
- Pediatrics: 2 Case ReportDocument50 pagesPediatrics: 2 Case ReportSam Raven AndresNo ratings yet
- Meningitis-Malaria E PDFDocument44 pagesMeningitis-Malaria E PDFSana ShafeeqNo ratings yet
- Acs TrombolitikDocument55 pagesAcs TrombolitikDiana IswardhaniNo ratings yet
- Ascitic Fluid AnalysisDocument3 pagesAscitic Fluid AnalysisLohJNo ratings yet
- Oral Revalida Im Cases Dec. 12 and 13 2020Document16 pagesOral Revalida Im Cases Dec. 12 and 13 2020Bea Y. Bas-ongNo ratings yet
- Diarrhea 2016Document37 pagesDiarrhea 2016oli garkiNo ratings yet
- Kelenjar LakrimalDocument44 pagesKelenjar LakrimalNurfanida Natasya MNo ratings yet
- Kawasaki Disease DiagnosisDocument5 pagesKawasaki Disease DiagnosisFranz SalazarNo ratings yet
- Acute Hypertension-Hypertensive Urgency and Hypertensive EmergencyDocument13 pagesAcute Hypertension-Hypertensive Urgency and Hypertensive EmergencyAmitKumarNo ratings yet
- Patient DT STEMI CaseDocument18 pagesPatient DT STEMI CaseZNo ratings yet
- Junior Intern NotesDocument3 pagesJunior Intern NotesTin SumangaNo ratings yet
- Deadly Kidney Infection: Understanding Emphysematous Pyelonephritis (EPNDocument31 pagesDeadly Kidney Infection: Understanding Emphysematous Pyelonephritis (EPNHardiTariqHammaNo ratings yet
- Pre-Op Case Protocol #4Document2 pagesPre-Op Case Protocol #4IC BNo ratings yet
- Viral Exanthem (Main)Document94 pagesViral Exanthem (Main)Starlet Rhonadez Bito-onon OrielNo ratings yet
- PulmoconDocument64 pagesPulmoconapi-3704562100% (1)
- How To Define CardiomegalyDocument2 pagesHow To Define CardiomegalyKjean De Vera MelendezNo ratings yet
- Bleed Vs Infarct ComparisonDocument7 pagesBleed Vs Infarct ComparisonJed ContrerasNo ratings yet
- Emergency Room Delivery RecordDocument7 pagesEmergency Room Delivery RecordMariel VillamorNo ratings yet
- Doctor's Medical OrdersDocument3 pagesDoctor's Medical OrdersAlyanna EvangelistaNo ratings yet
- Murmur EvaluationDocument4 pagesMurmur EvaluationManjunath GeminiNo ratings yet
- Lutembacher's Syndrome at KolonodaleDocument7 pagesLutembacher's Syndrome at KolonodaleWayan GunawanNo ratings yet
- Anginal Equivalents: Symptoms of Myocardial Ischemia Other Than Chest PainDocument6 pagesAnginal Equivalents: Symptoms of Myocardial Ischemia Other Than Chest PainGrant Wynn ArnucoNo ratings yet
- Surgery Case AppendicitisDocument30 pagesSurgery Case AppendicitisSarahNo ratings yet
- Pcap CSDocument21 pagesPcap CSKylie GolindangNo ratings yet
- Acute PancreatitisDocument11 pagesAcute PancreatitisChoirina QomariahNo ratings yet
- DR TahirDocument61 pagesDR TahirRohail GulNo ratings yet
- Cardiomyopathy My LectureDocument33 pagesCardiomyopathy My LectureAbraha HailuNo ratings yet
- Stroke and Cerebrovascular DiseaseDocument14 pagesStroke and Cerebrovascular DiseaseMarwan M.No ratings yet
- Congenital Heart DiseaseDocument124 pagesCongenital Heart DiseasemulkanmustafaNo ratings yet
- HepatomegalyDocument2 pagesHepatomegalyFuyumi RiaNo ratings yet
- Manage and Diagnose Acute and Chronic Cor PulmonaleDocument42 pagesManage and Diagnose Acute and Chronic Cor PulmonaleNym Angga SantosaNo ratings yet
- Acute Rheumatic Heart DiseaseDocument25 pagesAcute Rheumatic Heart DiseaseArun GeorgeNo ratings yet
- Acute Dyspnea First RevisionDocument56 pagesAcute Dyspnea First RevisionAradhanaRamchandaniNo ratings yet
- EKG PJK Co AssDocument115 pagesEKG PJK Co AsssalmaNo ratings yet
- Burn Injury PathophysiologyDocument1 pageBurn Injury PathophysiologyMonique Ann DanoyNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Contoh Presentasi Congenital Talipes EquinovarusDocument25 pagesContoh Presentasi Congenital Talipes EquinovarusFara OmarNo ratings yet
- Presentation Fraktur Distal Radius, Fraktur Styloid UlnaDocument23 pagesPresentation Fraktur Distal Radius, Fraktur Styloid UlnaFara OmarNo ratings yet
- VASCULARISASI EXTREMITAS ReviewDocument44 pagesVASCULARISASI EXTREMITAS ReviewFara OmarNo ratings yet
- Eritema Nodosum Necrotikan MH BL RFTDocument22 pagesEritema Nodosum Necrotikan MH BL RFTFara OmarNo ratings yet
- Ward Teaching "Drug Eruption"Document31 pagesWard Teaching "Drug Eruption"Fara OmarNo ratings yet
- Referensi Pediculosis PubisDocument4 pagesReferensi Pediculosis PubisFara OmarNo ratings yet
- Liver Tumors - Epidemiology, Diagnosis, Prevention and Treatment (Helen Reeves)Document184 pagesLiver Tumors - Epidemiology, Diagnosis, Prevention and Treatment (Helen Reeves)JohnQNo ratings yet
- Ten Weight Loss Tips To Swear by - DMoose FitnessDocument3 pagesTen Weight Loss Tips To Swear by - DMoose FitnessDMoose FitnessNo ratings yet
- Instant NoodlesDocument11 pagesInstant NoodlesBryan LeeNo ratings yet
- The Effects of Ice MassageDocument8 pagesThe Effects of Ice MassageCristopher Castro RdNo ratings yet
- Management of Pregnancy at RiskDocument40 pagesManagement of Pregnancy at RiskMA. JYRELL BONITONo ratings yet
- Juice Facts and Health EffectsDocument4 pagesJuice Facts and Health EffectsMuhamad Edho SyariffullahNo ratings yet
- Fluid and Electrolyte RegulationDocument94 pagesFluid and Electrolyte RegulationVergel RemorcaNo ratings yet
- ShackletonDocument27 pagesShackletonMontgomery2100% (2)
- Wa0011Document12 pagesWa0011Frengky AndikaNo ratings yet
- Listen to Your Body ClockDocument1 pageListen to Your Body ClockDavid BeckfilmNo ratings yet
- Inborn Errors of Lipid MetabolismDocument41 pagesInborn Errors of Lipid MetabolismWalterNo ratings yet
- Biologically Important Molecules Study Guide PDFDocument4 pagesBiologically Important Molecules Study Guide PDFsarahbeth1980No ratings yet
- Gestational Diabetes Mellitus Diagnosis and TreatmentDocument11 pagesGestational Diabetes Mellitus Diagnosis and TreatmentSadia YousafNo ratings yet
- Beta 3 Agonist SDocument9 pagesBeta 3 Agonist Slelouch_damienNo ratings yet
- Living Longer and Healthier LifeDocument233 pagesLiving Longer and Healthier Lifeweisberger100% (1)
- Aqa Byb1 W QP Jan04Document15 pagesAqa Byb1 W QP Jan04John SmithyNo ratings yet
- Raw Foods - Sept 2010Document32 pagesRaw Foods - Sept 2010vanitastarNo ratings yet
- Esophageal CancerDocument40 pagesEsophageal Cancerapi-282115150No ratings yet
- NNC Nutrition Devt Plan 2017 - 2022 PDFDocument15 pagesNNC Nutrition Devt Plan 2017 - 2022 PDFDulce Castillo-MoralesNo ratings yet
- FLL Research Paper RobokavsDocument10 pagesFLL Research Paper RobokavsRuth Carin - MalubayNo ratings yet
- Body Mass IndexDocument14 pagesBody Mass IndexAgnese NNo ratings yet
- Animal Nutrition: For Campbell Biology, Ninth EditionDocument74 pagesAnimal Nutrition: For Campbell Biology, Ninth EditionMahnoor AnjumNo ratings yet
- Banfield Pet Hospital State of Pet Health 2013 ReportDocument2 pagesBanfield Pet Hospital State of Pet Health 2013 ReportMichael_Lee_RobertsNo ratings yet
- Sesi 7c - Studi Kros Seksional 2011Document88 pagesSesi 7c - Studi Kros Seksional 2011rahimulyNo ratings yet
- Frequency RTB Free High-Frequency ProgramDocument68 pagesFrequency RTB Free High-Frequency ProgramMilena Molegno Marialuisa Riva CarrilloNo ratings yet
- NCM - Pregancy Induced HypertensionDocument5 pagesNCM - Pregancy Induced HypertensionZam PamateNo ratings yet
- SulfonylureasDocument3 pagesSulfonylureasarsalanzahid1No ratings yet
- Encyclopedia of Human Nutrition, Third Edition (PDFDrive)Document2,068 pagesEncyclopedia of Human Nutrition, Third Edition (PDFDrive)Fauziah Amrullah67% (3)
- Life 11 00532Document15 pagesLife 11 00532grpadillaNo ratings yet
- Junk Food PresentationDocument22 pagesJunk Food Presentationsuhas100% (1)