You might also like
- IESACDocument5 pagesIESACcnkamorevoleNo ratings yet
- Detect ADR Severity & CausesDocument4 pagesDetect ADR Severity & CausesRahmatulloh Al HusnaNo ratings yet
- DIS IPD Ceftriaxone KonsulDocument28 pagesDIS IPD Ceftriaxone KonsulTriana MaulidyahNo ratings yet
- Drug Therapy Assessment Worksheet (Dtaw) : 1. A Problem ExistsDocument6 pagesDrug Therapy Assessment Worksheet (Dtaw) : 1. A Problem ExistsputriNo ratings yet
- Case-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Document53 pagesCase-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Ditia RahimNo ratings yet
- D070415 PDFDocument5 pagesD070415 PDFRosyid PrasetyoNo ratings yet
- Farmakodinamik Obat Anti DiabetesDocument24 pagesFarmakodinamik Obat Anti DiabetesAsma Somadayo100% (1)
- Everything You Need to Know About Parenteral NutritionDocument31 pagesEverything You Need to Know About Parenteral NutritionNicholas PetrovskiNo ratings yet
- Materi 1 Dr. Apt. Diana Laila Ramatillah, M.farmDocument32 pagesMateri 1 Dr. Apt. Diana Laila Ramatillah, M.farmDimas RfNo ratings yet
- Leaflet - ProsoganDocument7 pagesLeaflet - ProsoganurmymelodyNo ratings yet
- Daftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiDocument28 pagesDaftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiDwiPrasetyaningRahmawatiNo ratings yet
- Gagal Ginjal Kuliah FarmakoterapiDocument39 pagesGagal Ginjal Kuliah FarmakoterapiriyuNo ratings yet
- Analysis of Adverse Effects of Anti-Tuberculosis DrugsDocument7 pagesAnalysis of Adverse Effects of Anti-Tuberculosis DrugsEva MelisaNo ratings yet
- To Ke 2 Apt 32Document101 pagesTo Ke 2 Apt 32Irma HastutiNo ratings yet
- Antibiotic Usage and DDD Analysis in Hospitalized PatientsDocument10 pagesAntibiotic Usage and DDD Analysis in Hospitalized PatientsJakobus Benny SalimNo ratings yet
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
- Antagonis Reseptor Angiotensin 2, AIIRADocument31 pagesAntagonis Reseptor Angiotensin 2, AIIRAsuho exoNo ratings yet
- Osteoarthritis: Degenerative Joint Disease - Prevalensi Meningkat Seiring DG Usia, Meningkat 2-10x DR Usia 30-65 THDocument58 pagesOsteoarthritis: Degenerative Joint Disease - Prevalensi Meningkat Seiring DG Usia, Meningkat 2-10x DR Usia 30-65 THbrevmanaNo ratings yet
- Percent removal of common antihypertensive drugs during hemodialysisDocument1 pagePercent removal of common antihypertensive drugs during hemodialysismazz.rianNo ratings yet
- DAFTAR OBAT ORAL PADAT BERDASARKAN KELAS FARMAKOTERAPI DAN FAST MOVINGDocument3 pagesDAFTAR OBAT ORAL PADAT BERDASARKAN KELAS FARMAKOTERAPI DAN FAST MOVINGlee andryNo ratings yet
- Daftar Obat Yang Dianjurkan Untuk Ibu Hamil Dan MenyusuiDocument10 pagesDaftar Obat Yang Dianjurkan Untuk Ibu Hamil Dan Menyusuisunar4deris5413No ratings yet
- Bailey - Deliver Trial Journal ClubDocument4 pagesBailey - Deliver Trial Journal Clubapi-665345625No ratings yet
- Daftar Pustaka: Drug Substances and ProductsDocument2 pagesDaftar Pustaka: Drug Substances and ProductsFaizah Min FadhlillahNo ratings yet
- Drug Related Problem Dan SOAP WordDocument18 pagesDrug Related Problem Dan SOAP WordIflakhatul UlfaNo ratings yet
- Dilution Guide For HAMDocument128 pagesDilution Guide For HAMummuawisyNo ratings yet
- Hipertensi Emergensi (Herbesser)Document41 pagesHipertensi Emergensi (Herbesser)riski novika100% (1)
- Permasalahan DLM CompoundingDocument60 pagesPermasalahan DLM CompoundingRusyda Humaira ArumaishaNo ratings yet
- Cost Analysis: Didik Setiawan, PHD., AptDocument20 pagesCost Analysis: Didik Setiawan, PHD., AptAnisaNo ratings yet
- Uji Bebas AlkoholDocument13 pagesUji Bebas AlkoholVieviepunya'esayonggRudii SakmampuseNo ratings yet
- 15 PharmaDocument32 pages15 PharmaGilbert OfeiNo ratings yet
- 10.preparasi TPN PDFDocument36 pages10.preparasi TPN PDFVini Insani RestuNo ratings yet
- Iohexol USP42NF37Document5 pagesIohexol USP42NF37John Alejandro Restrepo GarciaNo ratings yet
- Antibiotik Rasional Pada Demam TifoidDocument35 pagesAntibiotik Rasional Pada Demam TifoidSelvi SulistianingsihNo ratings yet
- Nama ObatDocument6 pagesNama ObatHelmalia PutriNo ratings yet
- Study of Adverse Drug Reactions Associated With Chemotherapy of Breast CancerDocument7 pagesStudy of Adverse Drug Reactions Associated With Chemotherapy of Breast CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Daftar Atc DDD Antibiotik Who 2018Document14 pagesDaftar Atc DDD Antibiotik Who 2018tri tanayawatiNo ratings yet
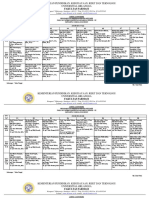
- Jadwal Ujian Sidang Periode 112 TGL 26-27 Juni 2021 (Rev)Document9 pagesJadwal Ujian Sidang Periode 112 TGL 26-27 Juni 2021 (Rev)Yohan Nafisa NetNo ratings yet
- Kinetik LengkapDocument133 pagesKinetik Lengkapreczky HasanNo ratings yet
- Usp Bud FactsheetDocument3 pagesUsp Bud FactsheetdellaNo ratings yet
- AST by The CDS Methode PDFDocument88 pagesAST by The CDS Methode PDFari_nuswantoroNo ratings yet
- KARAKTERISTIK TUGAS DAN TANGGUNG JAWAB APOTEKER MUSLIM - NewDocument30 pagesKARAKTERISTIK TUGAS DAN TANGGUNG JAWAB APOTEKER MUSLIM - NewBantuinAku KakNo ratings yet
- I. Farmakoterapi RasionalDocument24 pagesI. Farmakoterapi RasionalAthirah M.NoerNo ratings yet
- 2.tukak PeptikDocument42 pages2.tukak PeptikEfvi VhyLiaNo ratings yet
- Organization: Primary Business Address Address Line 2 Address Line 3 Address Line 4Document2 pagesOrganization: Primary Business Address Address Line 2 Address Line 3 Address Line 4celinangel100% (1)
- Farmakoterapi Coagulation DisorderDocument55 pagesFarmakoterapi Coagulation DisorderNur Astuty PurnamasariNo ratings yet
- (A) Pengembangan Obat - OBAT BIOLOGI - Ana Indrayati PDFDocument105 pages(A) Pengembangan Obat - OBAT BIOLOGI - Ana Indrayati PDFNugroho Wisnu PutroNo ratings yet
- Bio AssayDocument20 pagesBio AssayNeha Tiwari100% (2)
- SPO High AlerTDocument19 pagesSPO High AlerTHendraTriSaputroNo ratings yet
- Extending The Role of Pharmacists in Patient Care Are Pharmacists in Developing Nations Ready To ChangeDocument12 pagesExtending The Role of Pharmacists in Patient Care Are Pharmacists in Developing Nations Ready To Changebirhane gebreegziabiherNo ratings yet
- Bioavailabilitas & BioekivalenDocument27 pagesBioavailabilitas & Bioekivalendonghaesayangela100% (1)
- Drug Facts and Comparisons 2007Document2,136 pagesDrug Facts and Comparisons 2007Agus JiethoNo ratings yet
- Daftar Harga Buana Saraswati Bulan Agustus PDFDocument57 pagesDaftar Harga Buana Saraswati Bulan Agustus PDFJasa Sunat JembranaNo ratings yet
- Critical Appraisal Jurnal Asam Traneksamat Pada MelasmaDocument4 pagesCritical Appraisal Jurnal Asam Traneksamat Pada MelasmaMsrirrrNo ratings yet
- Swamed DiareDocument10 pagesSwamed DiaredhikaNo ratings yet
- Hyperkalemia & HypokalemiaDocument54 pagesHyperkalemia & Hypokalemiakhangsiean89No ratings yet
- MANAGEMENT OF HEPATOTOXIC POISONINGDocument66 pagesMANAGEMENT OF HEPATOTOXIC POISONINGnonoybenedictNo ratings yet
- Keto LogDocument7 pagesKeto LogKim Justin InfantadoNo ratings yet
- 10-Valproic AcidDocument49 pages10-Valproic AcidAli AmerNo ratings yet
- Management of DKA PresentationDocument46 pagesManagement of DKA PresentationMuhammed YesufNo ratings yet
- Physical Growth ControlDocument36 pagesPhysical Growth ControlchandununnaNo ratings yet
- Booklet MakanDocument36 pagesBooklet Makanryo_ninukNo ratings yet
- Proposal KesbangpolDocument7 pagesProposal Kesbangpolryo_ninukNo ratings yet
- (10)Document7 pages(10)ryo_ninukNo ratings yet
- Anemia DR ArwediDocument61 pagesAnemia DR Arwediryo_ninukNo ratings yet
- Physical Growth ControlDocument36 pagesPhysical Growth ControlchandununnaNo ratings yet
- PDFDocument6 pagesPDFryo_ninukNo ratings yet
- (5)Document9 pages(5)ryo_ninukNo ratings yet
- Methodology Checklist 2: Controlled Trials: Section 1: Internal ValidityDocument5 pagesMethodology Checklist 2: Controlled Trials: Section 1: Internal Validityryo_ninukNo ratings yet
- Age Ageing-2010-Lang-373-81Document9 pagesAge Ageing-2010-Lang-373-81ryo_ninukNo ratings yet
- Crystallization Kinetics of Coconut Oil Based On Avrami ModelDocument6 pagesCrystallization Kinetics of Coconut Oil Based On Avrami Modelryo_ninukNo ratings yet
- Hemodialysis Adequacy DwiDocument27 pagesHemodialysis Adequacy Dwiryo_ninukNo ratings yet
- Beers Criteria For Potentially Inappropriate MedicDocument3 pagesBeers Criteria For Potentially Inappropriate Medicryo_ninukNo ratings yet
- HD 2Document15 pagesHD 2ryo_ninukNo ratings yet
- Anticoagulant Wk4 FHMDocument21 pagesAnticoagulant Wk4 FHMryo_ninukNo ratings yet
- Optimal Time To Take Once-Daily Oral Medications in Clinical PracticeDocument18 pagesOptimal Time To Take Once-Daily Oral Medications in Clinical PracticeHerningtyas NLNo ratings yet
- Biodiversity, Ecology and Conservation BiologyDocument11 pagesBiodiversity, Ecology and Conservation Biologyryo_ninukNo ratings yet
- GL Radioph CGRPPDocument19 pagesGL Radioph CGRPPeduardodc777No ratings yet
- DVT GuidelineDocument1 pageDVT Guidelineryo_ninukNo ratings yet
- Numerical Modelling of Laterally Loaded Piles Captures Field Test ResponseDocument244 pagesNumerical Modelling of Laterally Loaded Piles Captures Field Test ResponseXiang ming GeNo ratings yet
- Fundamentals of VolleyballDocument2 pagesFundamentals of VolleyballLawrence CezarNo ratings yet
- Fe in Black TeaDocument6 pagesFe in Black TeaHerni Nur AeniNo ratings yet
- 7H17-28 Clearances and Wear Limits PDFDocument3 pages7H17-28 Clearances and Wear Limits PDFDimitris K100% (1)
- Total Tattoo-June 2021Document114 pagesTotal Tattoo-June 2021Comicgek100% (2)
- Earthbag House For HaitiDocument22 pagesEarthbag House For HaitiRaymond KatabaziNo ratings yet
- Carte Automatic TransmissionsDocument20 pagesCarte Automatic TransmissionsGigelNo ratings yet
- DG350 ManualDocument17 pagesDG350 ManualCareergamingNo ratings yet
- History of Cancer ChemotherapyDocument9 pagesHistory of Cancer ChemotherapyJoydeep MajumdarNo ratings yet
- VCDS Scan Reveals Faults in HVAC, ABS and Transmission SystemsDocument4 pagesVCDS Scan Reveals Faults in HVAC, ABS and Transmission SystemsDan MirceaNo ratings yet
- Ghost Events in Optical Time - NewDocument3 pagesGhost Events in Optical Time - NewsekutunetNo ratings yet
- Mouse Deer and TigerDocument2 pagesMouse Deer and Tigeralan.nevgan100% (1)
- 2 History of OrthodonticsDocument11 pages2 History of OrthodonticsMeiz JaleelNo ratings yet
- NQ-NQM Panelboards and Qonq Load Centers Information Manual 80043-712-06 Rev.02 06-2015 2 PiezasDocument144 pagesNQ-NQM Panelboards and Qonq Load Centers Information Manual 80043-712-06 Rev.02 06-2015 2 PiezasNadia EspinozaNo ratings yet
- AAA Variable Spring Hangers CatalogDocument31 pagesAAA Variable Spring Hangers CatalogNopparut0% (1)
- 2nd - Science-Second-Quarter-Week-1Document37 pages2nd - Science-Second-Quarter-Week-1Arlene AranzasoNo ratings yet
- Porter's Diamond Model Explains Nations' Success in IT CompetitionDocument30 pagesPorter's Diamond Model Explains Nations' Success in IT CompetitionKuthubudeen T MNo ratings yet
- EAGLE TUGS - Parts Service ManualDocument72 pagesEAGLE TUGS - Parts Service ManualDave MilnerNo ratings yet
- South African Flora GlossaryDocument47 pagesSouth African Flora Glossarymr.bryceNo ratings yet
- Paguro 06000 Spare Parts Catalogue PDFDocument88 pagesPaguro 06000 Spare Parts Catalogue PDFBoris Sitorus100% (2)
- Collab#2 (Edited)Document14 pagesCollab#2 (Edited)Yani BatoctoyNo ratings yet
- Kirloskar-Oil-Engines DescriptionsDocument8 pagesKirloskar-Oil-Engines Descriptionssinghhardeep760No ratings yet
- Life Below WaterDocument10 pagesLife Below Watertrisha sobito0% (1)
- Proceedings of National Conference on Landslides held in LudhianaDocument8 pagesProceedings of National Conference on Landslides held in LudhianaAniket PawarNo ratings yet
- PRN Maths Midterm QP Aug 18Document3 pagesPRN Maths Midterm QP Aug 18JanakChandPNo ratings yet
- Capacity and Safety Analysis of Hard Shoulder Running HSR A Motorway Case Study 2016 Transportation Research Part A Policy and PracticeDocument22 pagesCapacity and Safety Analysis of Hard Shoulder Running HSR A Motorway Case Study 2016 Transportation Research Part A Policy and PracticeZen ZeeNo ratings yet
- 1 s2.0 S2214860417301148 Main PDFDocument16 pages1 s2.0 S2214860417301148 Main PDFQuy Hoang KimNo ratings yet
- Polycab HT XlpeDocument33 pagesPolycab HT Xlpezafrikhan875No ratings yet
- Shakes Beer: Specialty CocktailsDocument2 pagesShakes Beer: Specialty CocktailsGilberto Luiz MeleiroNo ratings yet
- Refraction Through Lenses & Optical Instruments5Document144 pagesRefraction Through Lenses & Optical Instruments5geniusamahNo ratings yet