You might also like
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Bronchial AsthmaDocument71 pagesBronchial AsthmaHero MondaresNo ratings yet
- Bronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandBronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Childhood AsthmaDocument53 pagesChildhood AsthmaOlulode Olufemi S100% (1)
- Bronchitis Acute Brochitis: DefinitionDocument7 pagesBronchitis Acute Brochitis: DefinitionhemaanandhyNo ratings yet
- PneumothoraxDocument6 pagesPneumothoraxminmin69100% (1)
- Bronchitis: Kelompok IDocument14 pagesBronchitis: Kelompok ILinda Permata Sari100% (1)
- Bronchial AsthmaDocument64 pagesBronchial AsthmaDr. NasrumminallahNo ratings yet
- Tetralogy of FallotDocument10 pagesTetralogy of FallotanggiehardiyantiNo ratings yet
- EmphysemaDocument60 pagesEmphysemaJen Passilan100% (6)
- CopdDocument60 pagesCopdRizqy Shofianingrum100% (1)
- Lung AbsesDocument48 pagesLung AbsesAvhindAvhindNo ratings yet
- AsthmaDocument39 pagesAsthmamits98No ratings yet
- Pediatric Asthma PDFDocument12 pagesPediatric Asthma PDFzie_luph_taz13No ratings yet
- Bronchial AsthmaDocument22 pagesBronchial AsthmaJheric SbNo ratings yet
- Intestinal ObstructionDocument58 pagesIntestinal ObstructionTUSHAR PARMARNo ratings yet
- Bronchial AsthmaDocument71 pagesBronchial AsthmaQuolette Constante100% (1)
- Rheumatic Fever and RHDDocument49 pagesRheumatic Fever and RHDbereket gashuNo ratings yet
- Infective EndocarditiDocument31 pagesInfective EndocarditiMansi DabolaNo ratings yet
- Nursing Care of Bronchial AsthmaDocument16 pagesNursing Care of Bronchial AsthmaIntan RahmiNo ratings yet
- Management of Asthma ExacerbationDocument13 pagesManagement of Asthma ExacerbationAini Shofa HaniahNo ratings yet
- Bronchial Asthma: Harun ElçiçekDocument54 pagesBronchial Asthma: Harun ElçiçekFiras Ali100% (2)
- Bronchial AsthmaDocument29 pagesBronchial AsthmaDrShaheen100% (5)
- PneumoniaDocument86 pagesPneumoniamurugesh1969100% (1)
- PT Case: Copd Exacerbation: DedicationDocument10 pagesPT Case: Copd Exacerbation: DedicationDianaLopezBorjaNo ratings yet
- Ward Case PresentationDocument92 pagesWard Case PresentationSuzette Rae TateNo ratings yet
- Dr. K. V. Raman, Dean, MtpgrihsDocument66 pagesDr. K. V. Raman, Dean, MtpgrihsShruti100% (1)
- Guillain Barre SyndromeDocument5 pagesGuillain Barre SyndromeAriane Regalado100% (1)
- BRONCHITIS Case PresentationDocument28 pagesBRONCHITIS Case PresentationJoshua DulayNo ratings yet
- Lung AbscessDocument27 pagesLung AbscessMalueth Angui100% (1)
- Febrile SeizuresDocument23 pagesFebrile SeizuresHafiz FadhliNo ratings yet
- Bronchial AsthmaDocument23 pagesBronchial AsthmaAnna Carmela0% (1)
- Asthma!!!Document18 pagesAsthma!!!Jabbamackeez50% (2)
- Chronic BronchitisDocument11 pagesChronic BronchitisNazurah AzmiraNo ratings yet
- EmphysemaDocument3 pagesEmphysemaKhalid Mahmud ArifinNo ratings yet
- RBS and FBSDocument5 pagesRBS and FBSAllenne Rose Labja Vale100% (1)
- Neonatal SepsisDocument5 pagesNeonatal SepsisLeana SiñelNo ratings yet
- Pulmonary Tuberculosis 2016Document17 pagesPulmonary Tuberculosis 2016Nikka Moreen DagdagNo ratings yet
- Diarrhea: DefinitionDocument13 pagesDiarrhea: Definitionudaybujji100% (1)
- Case Study: Acute BronchitisDocument34 pagesCase Study: Acute BronchitisJeffany Anne Rabaya Retirado0% (1)
- CellulitisDocument15 pagesCellulitisSujatha J JayabalNo ratings yet
- Neurogenic Shock (New)Document14 pagesNeurogenic Shock (New)Syarafina AminuddinNo ratings yet
- Bronchial AsthmaDocument40 pagesBronchial Asthmasamson bd mokuntil100% (1)
- Care of Unconscious PatientDocument6 pagesCare of Unconscious PatientSuparna SinghaNo ratings yet
- Acute BronchitisDocument4 pagesAcute BronchitisLenjunNo ratings yet
- Pulmonary TuberculosisDocument17 pagesPulmonary TuberculosisRobert Dominic GonzalesNo ratings yet
- Case Presentation On Scrub TyphusDocument31 pagesCase Presentation On Scrub TyphusManojNo ratings yet
- Congenital Heart DiseaseDocument12 pagesCongenital Heart Diseaserakanootousan100% (1)
- COPDDocument30 pagesCOPDAmila SirisingheNo ratings yet
- PTB Case StudyDocument6 pagesPTB Case StudyTrisha Carolina SottoNo ratings yet
- PericarditisDocument45 pagesPericarditisBrenda WardshoneNo ratings yet
- COPD (Chronic Obstructive Pulmonary Disease)Document8 pagesCOPD (Chronic Obstructive Pulmonary Disease)Emily Anne86% (7)
- Case Study Tonsil It IsDocument16 pagesCase Study Tonsil It IsMuhammad FarhanNo ratings yet
- HydrocephalusDocument72 pagesHydrocephalusZharah RuzNo ratings yet
- Acute BronchitisDocument38 pagesAcute BronchitisNikko MelencionNo ratings yet
- Acute BronchitisDocument7 pagesAcute BronchitishqayqNo ratings yet
- Bronchitis ReportDocument34 pagesBronchitis ReportRolinette DaneNo ratings yet
- AsthmaDocument9 pagesAsthmaNiña Jemia CortezNo ratings yet
- Assignment Madam ZazaDocument5 pagesAssignment Madam Zazanur syafiqah kamaruzamanNo ratings yet
- Psychiatric Case StudyDocument32 pagesPsychiatric Case Studyrachael85% (33)
- (Roche-Dialysis Expert Workshop) Optimizing The Treatment of Renal Anemia. 100412Document28 pages(Roche-Dialysis Expert Workshop) Optimizing The Treatment of Renal Anemia. 100412nur syafiqah kamaruzamanNo ratings yet
- Power Point IHDDocument143 pagesPower Point IHDnur syafiqah kamaruzamanNo ratings yet
- Colles FractureDocument89 pagesColles Fracturenur syafiqah kamaruzaman100% (1)
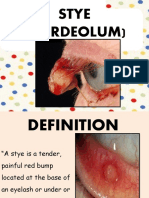
- StyeDocument21 pagesStyenur syafiqah kamaruzamanNo ratings yet
- Chicken Pox PresentationDocument14 pagesChicken Pox Presentationnur syafiqah kamaruzaman100% (3)
- Program of Instruction First Aid With MciDocument10 pagesProgram of Instruction First Aid With MciShan Dave TupasNo ratings yet
- Moran CORE - How To Use The Direct OphthalmoscopeDocument1 pageMoran CORE - How To Use The Direct OphthalmoscopeSamsung M20APNo ratings yet
- CystosDocument1 pageCystosgeorgeloto12No ratings yet
- Radiologi Kedaruratan & Traumatologi-Prof. Dr. Bachtiar MDocument55 pagesRadiologi Kedaruratan & Traumatologi-Prof. Dr. Bachtiar MMonazzt AsshagabNo ratings yet
- 1 BarashDP - Paradigms Lost AbridgedDocument7 pages1 BarashDP - Paradigms Lost AbridgedFABIONo ratings yet
- 95 Formulation and Evaluation of Diclofenac Sodium Gel by Using Natural PolymerDocument3 pages95 Formulation and Evaluation of Diclofenac Sodium Gel by Using Natural PolymerJulian Kayne100% (1)
- Raja Nigantu IntroductionDocument8 pagesRaja Nigantu IntroductionMedico PassNo ratings yet
- Chin Chong MinDocument3 pagesChin Chong MinSHine PukurNo ratings yet
- Physician To Population Ratios Physician Supply StandardsDocument5 pagesPhysician To Population Ratios Physician Supply StandardsjackeldescargadorNo ratings yet
- Raw Materials & Purification - NitrogenDocument9 pagesRaw Materials & Purification - Nitrogensexyrusty0% (1)
- RXN For DR - SagamlaDocument2 pagesRXN For DR - Sagamlayeng botzNo ratings yet
- Nine Principles For Improved Nurse Staffing by Bob DentDocument6 pagesNine Principles For Improved Nurse Staffing by Bob DentJennyLapitanNo ratings yet
- 40 Sa Hindi - LBDocument6 pages40 Sa Hindi - LBIrshad mohammedNo ratings yet
- Simultaneous Determination of Methylparaben + Propylparaben + Hidrocortisone Topical Cream PDFDocument7 pagesSimultaneous Determination of Methylparaben + Propylparaben + Hidrocortisone Topical Cream PDFNájla KassabNo ratings yet
- Metoprolol and AmiodaroneDocument5 pagesMetoprolol and AmiodaroneNolte BombayNo ratings yet
- The Menstrual Cycle Remedies Amenorrhea HandoutDocument3 pagesThe Menstrual Cycle Remedies Amenorrhea HandoutRoger AugeNo ratings yet
- Clinical Case Studies 2007 Townend 443 53Document12 pagesClinical Case Studies 2007 Townend 443 53cioaca12No ratings yet
- David Blaine BiographyDocument7 pagesDavid Blaine BiographyPunkaj YadavNo ratings yet
- Primary Awards 2012-2014 - CaribbeansDocument7 pagesPrimary Awards 2012-2014 - CaribbeansGuillaume PrefolNo ratings yet
- 7 Uses For Medical MarijuanaDocument4 pages7 Uses For Medical MarijuanaYhojan Surco ZavalaNo ratings yet
- TheraSuit BrochureDocument8 pagesTheraSuit BrochureMhmd IrakyNo ratings yet
- Legal MedDocument42 pagesLegal Medaisajane_rmt100% (6)
- Research EssasyDocument9 pagesResearch Essasyapi-279881900No ratings yet
- Pathogenesis of PcosDocument14 pagesPathogenesis of PcosMitali Narurkar100% (1)
- Case Study - 4 FractureDocument35 pagesCase Study - 4 FracturekavindukarunarathnaNo ratings yet
- AspirinDocument11 pagesAspirinAffie OtunlaNo ratings yet
- Tushar FinalDocument29 pagesTushar FinalRaj Prixit RathoreNo ratings yet
- Part 1 - Bernal Safety - Intro and Emergencies - Powerpoint - 29mar21Document34 pagesPart 1 - Bernal Safety - Intro and Emergencies - Powerpoint - 29mar21John TorrezNo ratings yet
- Contents (Continued) : Chapter 5. Nondestructive Inspection (Ndi)Document3 pagesContents (Continued) : Chapter 5. Nondestructive Inspection (Ndi)blackhawkNo ratings yet
- Acute Limb Ischemia: Clinical PracticeDocument9 pagesAcute Limb Ischemia: Clinical PracticeIndah MaulidawatiNo ratings yet