You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Differential Diagnosis of Most Common Symptoms - DR - AhmadosDocument2 pagesDifferential Diagnosis of Most Common Symptoms - DR - AhmadosRashed ShatnawiNo ratings yet
- My Cardiac and Chest SymptomsDocument58 pagesMy Cardiac and Chest SymptomsDhamirah SakinahNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- الباطنة كلها بالتفصيل في 160 صفحة فقط لازم تحمل المذكرة فوراDocument163 pagesالباطنة كلها بالتفصيل في 160 صفحة فقط لازم تحمل المذكرة فورانادين مطر0% (1)
- History Taking 2. Physical Examination 3. Diagnostic TestsDocument33 pagesHistory Taking 2. Physical Examination 3. Diagnostic TestsAmalNo ratings yet
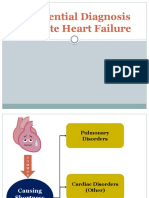
- LI 8 - Differential Diagnosis of Acute Heart FailureDocument11 pagesLI 8 - Differential Diagnosis of Acute Heart Failure19-034 Jefry Junaidi PurbaNo ratings yet
- Research MethodsDocument8 pagesResearch MethodsSilver DrakeNo ratings yet
- Toronto Notes Respirology PDFDocument40 pagesToronto Notes Respirology PDFJaya Semara Putra67% (3)
- AirwayDocument2 pagesAirwayKaitlynHynes34No ratings yet
- Sypmtoms and Signs of Respiratory DiseasesDocument22 pagesSypmtoms and Signs of Respiratory DiseasesPrincewill SeiyefaNo ratings yet
- Respiratory Failure: by Amera GumamaDocument26 pagesRespiratory Failure: by Amera GumamaGumama AmeiyrhaNo ratings yet
- Medical Semiology Respiratory SystemDocument111 pagesMedical Semiology Respiratory SystemNadir al bu lahNo ratings yet
- Cardiology-7 MEDIASTDocument19 pagesCardiology-7 MEDIASTMahmoud RamadanNo ratings yet
- Understanding Respiratory FailureDocument134 pagesUnderstanding Respiratory FailureFirdaus AldyNo ratings yet
- Understanding Respiratory Failure: Causes, Symptoms, Diagnosis and TreatmentDocument49 pagesUnderstanding Respiratory Failure: Causes, Symptoms, Diagnosis and TreatmentimaderadityaNo ratings yet
- Essential Basics of General Medicine Faculty of Dentistry Cairo UniversityDocument104 pagesEssential Basics of General Medicine Faculty of Dentistry Cairo Universitybavly waidyNo ratings yet
- Lung Examination Guide: Physical Steps, Pathologies, Dyspnea TypesDocument145 pagesLung Examination Guide: Physical Steps, Pathologies, Dyspnea TypesIrina CornilovNo ratings yet
- Dyspnea PresentationDocument37 pagesDyspnea PresentationamgoperaNo ratings yet
- DyspnoeaDocument1 pageDyspnoeaShubham TarapureNo ratings yet
- 2 - Dyspnea 讲课稿 2020Document16 pages2 - Dyspnea 讲课稿 2020mirabel IvanaliNo ratings yet
- HemoptysisDocument32 pagesHemoptysisbudiNo ratings yet
- Mitral StenosisDocument19 pagesMitral StenosisAbdur RaqibNo ratings yet
- Churchill's Pocketbook of Differential Diagnosis, Fourth EditionDocument6 pagesChurchill's Pocketbook of Differential Diagnosis, Fourth EditionalexisNo ratings yet
- Acute & Chronic Bronchitis & COPDDocument49 pagesAcute & Chronic Bronchitis & COPDHendraDarmawanNo ratings yet
- Tutor 1 Blok 13-14Document109 pagesTutor 1 Blok 13-14Jericho ImmanuelaNo ratings yet
- Case Presentation On Chest PainDocument36 pagesCase Presentation On Chest PainpayumoNo ratings yet
- PATHOPHYSIOLOGYDocument46 pagesPATHOPHYSIOLOGYnimrakhalid82000No ratings yet
- 13 - Lung PathologyDocument38 pages13 - Lung PathologyRodriguez Vivanco Kevin DanielNo ratings yet
- History TakingDocument28 pagesHistory TakingYeniNo ratings yet
- Respiratory System History Taking: Dr. Aiman Al ShareiDocument20 pagesRespiratory System History Taking: Dr. Aiman Al ShareiQusai IbraheemNo ratings yet
- Breathlessness: Causes, Evaluation and ManagementDocument10 pagesBreathlessness: Causes, Evaluation and ManagementAckNo ratings yet
- 5. Hemoptysis 讲稿Document4 pages5. Hemoptysis 讲稿mirabel IvanaliNo ratings yet
- Pulmonary Hypertension: An Overview of Causes, Symptoms and DiagnosisDocument40 pagesPulmonary Hypertension: An Overview of Causes, Symptoms and DiagnosisAlexander Santiago ParelNo ratings yet
- Clinical Physiology of Respiration: Dr. M Qathar RF TDocument76 pagesClinical Physiology of Respiration: Dr. M Qathar RF TTiwi Lestari TiwiNo ratings yet
- Acute Respiratory FailureDocument8 pagesAcute Respiratory FailureCayunk NorlianaNo ratings yet
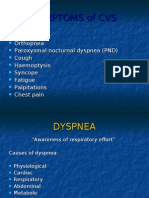
- Symptoms of CvsDocument25 pagesSymptoms of CvsstudymedicNo ratings yet
- Key signs and symptoms of respiratory diseasesDocument35 pagesKey signs and symptoms of respiratory diseasesEmereole FrancesNo ratings yet
- Approach To Cough and HemoptysisDocument24 pagesApproach To Cough and Hemoptysisbansaleliza26No ratings yet
- Respirotary MnemonicsDocument9 pagesRespirotary MnemonicsAymen Omer0% (1)
- 20) PericarditisDocument3 pages20) PericarditisAris PaparisNo ratings yet
- Cor PulmonaleDocument22 pagesCor PulmonaleRianda Dwi PutraNo ratings yet
- Cardio AssessmentDocument118 pagesCardio AssessmentNashrina NashrinaNo ratings yet
- Sindromatologi DyspneuDocument18 pagesSindromatologi DyspneuMeylan TaebenuNo ratings yet
- Pneumothorax and Pneumomediastinum: Dr. Emad EfatDocument89 pagesPneumothorax and Pneumomediastinum: Dr. Emad Efatinterna MANADONo ratings yet
- Chest Pain and Dyspnea CausesDocument12 pagesChest Pain and Dyspnea CausesAmi DhaniaNo ratings yet
- NAME: Neema Tamang Roll No:-20 Subject:-Surgery Assignment Topic:-Pneumothorax Faculty: HA 2Document9 pagesNAME: Neema Tamang Roll No:-20 Subject:-Surgery Assignment Topic:-Pneumothorax Faculty: HA 2Shreekrishna BudhathokiNo ratings yet
- An Approach To A Patient With BreathlessnessDocument35 pagesAn Approach To A Patient With Breathlessnessgl tousifNo ratings yet
- Intractable, Refractory Cough - Jindal IVF ChandigarhDocument9 pagesIntractable, Refractory Cough - Jindal IVF ChandigarhJindal Chest ClinicNo ratings yet
- NCM 112 LEC Topic 9 Respiratory Distress Syndrome RDSDocument4 pagesNCM 112 LEC Topic 9 Respiratory Distress Syndrome RDSViviene Faye FombuenaNo ratings yet
- 1 ClubbingDocument10 pages1 Clubbingnathanaellee92No ratings yet
- Causes, Symptoms and Diagnosis of Pleural EffusionDocument8 pagesCauses, Symptoms and Diagnosis of Pleural EffusionerrickaiNo ratings yet
- Chronic Obstructive Disease by HibaDocument38 pagesChronic Obstructive Disease by HibahibaNo ratings yet
- Notes SC RSDocument5 pagesNotes SC RS202213No ratings yet
- Sesak Napas Arimbi (PBL)Document50 pagesSesak Napas Arimbi (PBL)Endik SiswantoNo ratings yet
- Systemic Disorders of The LungDocument74 pagesSystemic Disorders of The Lungjhay-r reyesNo ratings yet
- Inflammation of Any Layer of Heart (Endo, Myo, Peri) : Damaging Valves, Muscles and /or Pericardial LiningsDocument15 pagesInflammation of Any Layer of Heart (Endo, Myo, Peri) : Damaging Valves, Muscles and /or Pericardial LiningsNur SetsuNo ratings yet
- Interstitial Lung Diseases (Ild)Document40 pagesInterstitial Lung Diseases (Ild)TaufiqHidayatRidwanNo ratings yet
- Medicine RespiratoryDocument53 pagesMedicine RespiratoryMohiuddin AhmedNo ratings yet
- Protein and Its MythDocument5 pagesProtein and Its MythRaushan BlakeNo ratings yet
- Om Algora SLE Exam-2 PDFDocument496 pagesOm Algora SLE Exam-2 PDFGomathy DhanasekarNo ratings yet
- Cardiovascular Complications of Down Syndrome Scoping Review and Expert Consensus PDFDocument17 pagesCardiovascular Complications of Down Syndrome Scoping Review and Expert Consensus PDFDaniela Peinado RiosNo ratings yet
- Odontoterapie Anul III EnglezaDocument25 pagesOdontoterapie Anul III EnglezaEugen Secher0% (1)
- Periodontal Surgery ClassificationDocument4 pagesPeriodontal Surgery ClassificationRinisha SinhaNo ratings yet
- Debre Markos University Epidemiology ScreeningDocument55 pagesDebre Markos University Epidemiology ScreeningTewodros AntenehNo ratings yet
- Abnormal Psychology - Past and PresentDocument19 pagesAbnormal Psychology - Past and PresentRizwana MBTNo ratings yet
- Surgical ConscienceDocument35 pagesSurgical ConscienceTakale BuloNo ratings yet
- DineshPonraj 1808165 - 05 00 - 1Document4 pagesDineshPonraj 1808165 - 05 00 - 1revanth kumarNo ratings yet
- Kejahatan SeksualDocument12 pagesKejahatan SeksualachyarininoviolaNo ratings yet
- 21Document7 pages21pangetkoNo ratings yet
- ENGLISH10-QTR4-LAS-MELC-3Document8 pagesENGLISH10-QTR4-LAS-MELC-3jhanceedebbieNo ratings yet
- Malaria: Michael Aguilar, RMTDocument27 pagesMalaria: Michael Aguilar, RMTFrankenstein MelancholyNo ratings yet
- Cortical Visual Impairment and Blindness: by Komal SharmaDocument15 pagesCortical Visual Impairment and Blindness: by Komal SharmaOphthalmology DiscussionNo ratings yet
- The Major Effects of Covid-19 in The PhilippinesDocument8 pagesThe Major Effects of Covid-19 in The PhilippinesRafael ArchieNo ratings yet
- Palliative Nursing CareDocument1 pagePalliative Nursing Carenurwanda hamidaNo ratings yet
- Fluticasone Drug StudyDocument3 pagesFluticasone Drug StudyArabelle GONo ratings yet
- Eau Guidelines On Urological Infections: (Limited Text Update March 2022)Document27 pagesEau Guidelines On Urological Infections: (Limited Text Update March 2022)Andrea Romano ForcinitiNo ratings yet
- Lip BumperDocument60 pagesLip BumperPînzariu GeorgeNo ratings yet
- 2ND Exam Part 2Document5 pages2ND Exam Part 2SajeebChandraNo ratings yet
- 10 Ways To Boost Male Fertility and Increase Sperm CountDocument12 pages10 Ways To Boost Male Fertility and Increase Sperm Countahmed hassanNo ratings yet
- Toy Enc 1102 Spring2021Document25 pagesToy Enc 1102 Spring2021api-355676368No ratings yet
- 150 Question & Answer in EndoDocument21 pages150 Question & Answer in EndoDarwin Nunez100% (2)
- Covid-19 Case Study Using MS-Excel (Report) : Submitted By: Rasika Deshpande (020) PGDM-RBA, Welingkar, BangaloreDocument19 pagesCovid-19 Case Study Using MS-Excel (Report) : Submitted By: Rasika Deshpande (020) PGDM-RBA, Welingkar, BangaloreRasika DeshpandeNo ratings yet
- Padua Inventory - Washington State University RevisionDocument3 pagesPadua Inventory - Washington State University RevisionlaiaNo ratings yet
- Hi Yield Goljan Pathology Review MemorizeDocument57 pagesHi Yield Goljan Pathology Review MemorizeTrisNo ratings yet
- Application of Eye Patch, Shield and Bandage.Document19 pagesApplication of Eye Patch, Shield and Bandage.yaraNo ratings yet
- J. Biol. Chem.-2020-Traughber-8252-61Document11 pagesJ. Biol. Chem.-2020-Traughber-8252-61exoNo ratings yet
- Pin Ikabdi 2022Document18 pagesPin Ikabdi 2022Kevin AdrianNo ratings yet
- 2023 Identifying Risk of Death in Children Hospitalized With Community-Acquired PneumoniaDocument9 pages2023 Identifying Risk of Death in Children Hospitalized With Community-Acquired PneumoniaOlga CîrsteaNo ratings yet