You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 04.02 Assignment FinishedDocument5 pages04.02 Assignment Finishedjazzmine andesonNo ratings yet
- Management of Hypertension-Hypotension in The ERDocument79 pagesManagement of Hypertension-Hypotension in The ERdkhandkeNo ratings yet
- Themes of World Kidney Day-2018Document25 pagesThemes of World Kidney Day-2018dkhandkeNo ratings yet
- PPAR in CVSDocument32 pagesPPAR in CVSdkhandkeNo ratings yet
- ImidapriDocument6 pagesImidapriLinda Rusliana SariNo ratings yet
- BetaBlockers RevisitedDocument8 pagesBetaBlockers RevisiteddkhandkeNo ratings yet
- Complete Guide to Anemia-Free PregnancyDocument39 pagesComplete Guide to Anemia-Free PregnancydkhandkeNo ratings yet
- Antiplatelet Therapy For Acute Coronary SyndromeDocument105 pagesAntiplatelet Therapy For Acute Coronary SyndromedkhandkeNo ratings yet
- Cilnidipine 1Document62 pagesCilnidipine 1dkhandke0% (1)
- ADA Update 2014Document53 pagesADA Update 2014dkhandkeNo ratings yet
- Antiplatelet Therapy For Acute Coronary SyndromeDocument105 pagesAntiplatelet Therapy For Acute Coronary SyndromedkhandkeNo ratings yet
- Optimizing Therapy in Heart Failure 1-FinalDocument52 pagesOptimizing Therapy in Heart Failure 1-FinaldkhandkeNo ratings yet
- Resistant Hypertension evaluation and managementDocument56 pagesResistant Hypertension evaluation and managementdkhandkeNo ratings yet
- New Relevance of Roxithromycin - An Emerging Therapeutic ApproachDocument30 pagesNew Relevance of Roxithromycin - An Emerging Therapeutic ApproachdkhandkeNo ratings yet
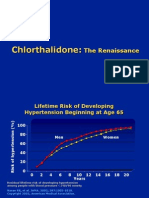
- Chlorthalidone-Telmisartan The New RenaissanceDocument127 pagesChlorthalidone-Telmisartan The New Renaissancedkhandke100% (1)
- ADA Update 2014Document53 pagesADA Update 2014dkhandkeNo ratings yet
- Hypertension An OverviewDocument214 pagesHypertension An OverviewdkhandkeNo ratings yet
- How To Read A Clinical PaperDocument76 pagesHow To Read A Clinical PaperdkhandkeNo ratings yet
- Skeletal TractionDocument11 pagesSkeletal Tractionpolarbear121212No ratings yet
- Study On Effect of Wet Cupping (Hijama) On Blood Lipid Profile in Human at Aldyssah-Alshati, LibyaDocument4 pagesStudy On Effect of Wet Cupping (Hijama) On Blood Lipid Profile in Human at Aldyssah-Alshati, LibyaMohammed Ramzy GhifariNo ratings yet
- PolicyDocument8 pagesPolicyjoshiaruna539No ratings yet
- Piriformis SyndromeDocument6 pagesPiriformis SyndromeChân Mệnh Thiên TửNo ratings yet
- Beyond Bowels: Understanding Co-existing Symptoms in IBSDocument8 pagesBeyond Bowels: Understanding Co-existing Symptoms in IBSparthibanemails5779No ratings yet
- Physical & Multiple Disability ChecklistDocument3 pagesPhysical & Multiple Disability ChecklistGheylhu AmorNo ratings yet
- IV Drug ReactionsDocument19 pagesIV Drug Reactionsphp_czarina04421No ratings yet
- Eye Care ProcedureDocument9 pagesEye Care ProcedureSharon Lawrence100% (1)
- History of Microbiology-Notes For QuizDocument20 pagesHistory of Microbiology-Notes For QuizPipay AllenaNo ratings yet
- Overview of Digestive System 16-01-23Document20 pagesOverview of Digestive System 16-01-23erisericssonNo ratings yet
- Circulatory SystemDocument21 pagesCirculatory SystemYusuf AzeezNo ratings yet
- Chapter 2, Collecting Subjective DataDocument8 pagesChapter 2, Collecting Subjective DataEmvie Loyd Pagunsan-ItableNo ratings yet
- Review of Influenza as a Seasonal and Pandemic DiseaseDocument12 pagesReview of Influenza as a Seasonal and Pandemic DiseaseFreddy SueroNo ratings yet
- Breast MCQDocument13 pagesBreast MCQMahmoud Abouelsoud100% (1)
- Data Obat Lengkap-SIAP IMPORTDocument9 pagesData Obat Lengkap-SIAP IMPORTRegita Ragil SejahteraNo ratings yet
- Alee Resume 2 23Document2 pagesAlee Resume 2 23api-624592395No ratings yet
- Rice DiseaseDocument23 pagesRice DiseaseRayge HarbskyNo ratings yet
- MdsDocument570 pagesMdsAgus SusantoNo ratings yet
- Designated Medical Event Dme List enDocument3 pagesDesignated Medical Event Dme List enAmany HagageNo ratings yet
- Success Manual and Cheat Sheet Notes To Pass Your Basic Life Support (BLS) CourseDocument11 pagesSuccess Manual and Cheat Sheet Notes To Pass Your Basic Life Support (BLS) CourseanthonyNo ratings yet
- Breast Augmentation and Breast ReductionDocument13 pagesBreast Augmentation and Breast ReductionDjlatino LatinoNo ratings yet
- 8 Sports Injury ManagementDocument21 pages8 Sports Injury ManagementPatch04No ratings yet
- Critical care guidelines for IV nicardipine useDocument3 pagesCritical care guidelines for IV nicardipine useLisa Trisnawati ChaniagoNo ratings yet
- Nosocomial Infection?Document4 pagesNosocomial Infection?Sara ANo ratings yet
- Diastema Closure PDFDocument5 pagesDiastema Closure PDFsimon yonathanNo ratings yet
- Test Bank For Maternity and Womens Health Care 12th Edition Deitra Leonard Lowdermilk Shannon e Perry Mary Catherine Cashion Kathryn Rhodes Alden Ellen OlshanskyDocument9 pagesTest Bank For Maternity and Womens Health Care 12th Edition Deitra Leonard Lowdermilk Shannon e Perry Mary Catherine Cashion Kathryn Rhodes Alden Ellen Olshanskysubitodomesticcz70o3No ratings yet
- ZIKA 101: CDC'S Response To ZikaDocument54 pagesZIKA 101: CDC'S Response To ZikaShirley MendezNo ratings yet
- Grafton Campus MapDocument1 pageGrafton Campus MapPUSKESMAS KECAMATAN KEPULAUAN SERIBU UTARANo ratings yet
- Management of Post-Operative Nausea and Vomiting in Adults - The Pharmaceutical JournalDocument18 pagesManagement of Post-Operative Nausea and Vomiting in Adults - The Pharmaceutical JournalResti DwiuNo ratings yet