You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Misra U, Kalita J Dan Dubey D. A Study of Super Refractory Status Epilepticus From IndiaDocument10 pagesMisra U, Kalita J Dan Dubey D. A Study of Super Refractory Status Epilepticus From IndiasitialimahNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Donker Kaat, LauraDocument182 pagesDonker Kaat, LaurasitialimahNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Siti Pembahasan Lokasi, Dan Jenis StrokeDocument1 pageSiti Pembahasan Lokasi, Dan Jenis StrokesitialimahNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Neurosurg Focus Article PE4Document10 pagesNeurosurg Focus Article PE4sitialimahNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- 171 183Document13 pages171 183dianNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptsitialimahNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Therapy Ocular ToxoplasmosisDocument8 pagesTherapy Ocular ToxoplasmosissitialimahNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Coagulation in Brain RumorDocument9 pagesCoagulation in Brain RumorsitialimahNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 951 FullDocument6 pages951 FullsitialimahNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptsitialimahNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Manejo Del SGB 10 PasosDocument13 pagesManejo Del SGB 10 PasosRonald ReyesNo ratings yet
- TNOAJOphthalmicSciRes56271-4396733 121247halfDocument6 pagesTNOAJOphthalmicSciRes56271-4396733 121247halfsitialimahNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Maschio Et Al (2019) Management of Epilelsy in Brain TumorsDocument18 pagesMaschio Et Al (2019) Management of Epilelsy in Brain TumorssitialimahNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- SOP Myasthenic Crisis: Standardoperatingprocedure Open AccessDocument6 pagesSOP Myasthenic Crisis: Standardoperatingprocedure Open AccesssitialimahNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Wong TY Mitchell P Editors 2004 Current Concept Hypertensive RetinopathyDocument8 pagesWong TY Mitchell P Editors 2004 Current Concept Hypertensive Retinopathychaer assofiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Serotonin Syndrome: Pathophysiology, Clinical Features, Management, and Potential Future DirectionsDocument14 pagesSerotonin Syndrome: Pathophysiology, Clinical Features, Management, and Potential Future DirectionssitialimahNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Shoulder Pain 3Document8 pagesShoulder Pain 3sitialimahNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Controversial diagnosis and management of serotonin syndromeDocument3 pagesControversial diagnosis and management of serotonin syndromeWaqas ShahnawazNo ratings yet
- Shoulder - Pain - Diagnosis - and - Management - in - Primary 3Document6 pagesShoulder - Pain - Diagnosis - and - Management - in - Primary 3sitialimahNo ratings yet
- MastersDocument6 pagesMastersAnonymous ckZmIgoNo ratings yet
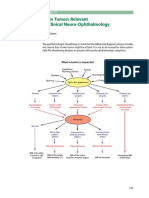
- Ophthalmic Manifestations in Patients With IntracrDocument9 pagesOphthalmic Manifestations in Patients With IntracrsitialimahNo ratings yet
- Visual Findings As Primary Manifestations in Patients With Intracranial TumorsDocument4 pagesVisual Findings As Primary Manifestations in Patients With Intracranial TumorsScoalaAuto AutoSorNo ratings yet
- Dolor Hombro Evaluacion Tto PDFDocument18 pagesDolor Hombro Evaluacion Tto PDFAnonymous ckZmIgoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2017 Rehab ShoulderDocument11 pages2017 Rehab ShoulderRizka ApNo ratings yet
- 11 Cai Et, Al., 2020) Being at Risk of Malnutrition Predicts Poor Outcomes at 3 Months in Acute Ischemic Stroke PatientsDocument10 pages11 Cai Et, Al., 2020) Being at Risk of Malnutrition Predicts Poor Outcomes at 3 Months in Acute Ischemic Stroke PatientssitialimahNo ratings yet
- (12 Y, Shiga, T. Nezu, 2019) Effect of Tooth Loss and Nutritional Status On Outcomes After Ischemic Stroke. NutritionDocument24 pages(12 Y, Shiga, T. Nezu, 2019) Effect of Tooth Loss and Nutritional Status On Outcomes After Ischemic Stroke. NutritionsitialimahNo ratings yet
- (10 Xiang W, Chen X, 2020) Prognostic Nutritional Index For Predicting 3-Month Outcomes in Ischemic Stroke Patients Undergoing ThrombolyDocument7 pages(10 Xiang W, Chen X, 2020) Prognostic Nutritional Index For Predicting 3-Month Outcomes in Ischemic Stroke Patients Undergoing ThrombolysitialimahNo ratings yet
- (2 Zhang Et, Al. 2016) Prevalence of Stroke and Associated Risk Factors A Population Based Cross Sectional Study From Northeast ChinaDocument11 pages(2 Zhang Et, Al. 2016) Prevalence of Stroke and Associated Risk Factors A Population Based Cross Sectional Study From Northeast ChinasitialimahNo ratings yet
- Pathophysiology and Treatment of Stroke: Present Status and Future PerspectivesDocument24 pagesPathophysiology and Treatment of Stroke: Present Status and Future Perspectivesdewinta fitriNo ratings yet
- (1 Bender, Et Al 2017) High Burden of Stroke Risk Factors in Developing Country The Case Study of BosniaDocument3 pages(1 Bender, Et Al 2017) High Burden of Stroke Risk Factors in Developing Country The Case Study of BosniasitialimahNo ratings yet
- People Vs Peralta, Et AlDocument3 pagesPeople Vs Peralta, Et AlRR FNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Mug Ruith Beheads The Prophet PDFDocument2 pagesMug Ruith Beheads The Prophet PDFPeteJH2014No ratings yet
- Horror story pillow parasite drains woman's bloodDocument9 pagesHorror story pillow parasite drains woman's bloodwmmcgregor93No ratings yet
- Reflection Paper About DeathDocument2 pagesReflection Paper About DeathHermelyn EsparagozaNo ratings yet
- Anauria Asram Hlondath by PhasaiDocument63 pagesAnauria Asram Hlondath by Phasaiadam kyser100% (4)
- How To Say Rosary - LatinDocument2 pagesHow To Say Rosary - LatingbpadillajrNo ratings yet
- Insurance Commission ReviewerDocument29 pagesInsurance Commission Reviewerabi horohoroNo ratings yet
- April 30 Crim DigestsDocument355 pagesApril 30 Crim Digestspinkblush717No ratings yet
- تحليلية الترجمة أولى ماستر د,شليDocument4 pagesتحليلية الترجمة أولى ماستر د,شليMohamed DEZIRINo ratings yet
- Britt A. Bunyard: Key Words: Amanita, AmanitaDocument4 pagesBritt A. Bunyard: Key Words: Amanita, AmanitajakwiNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 12th English Ch.2 The Tiger KingDocument3 pages12th English Ch.2 The Tiger KingRachit KumarNo ratings yet
- OC Register March 13, 1995 - 3 of 3Document1 pageOC Register March 13, 1995 - 3 of 3Kathryn C. GeierNo ratings yet
- Mr. Rizal (Story of Mi Ultimo Adios) - Jan-19-2015 (MJS)Document14 pagesMr. Rizal (Story of Mi Ultimo Adios) - Jan-19-2015 (MJS)Jam Silverio50% (2)
- Quick Notes of Forensic Medicine and ToxicologyDocument13 pagesQuick Notes of Forensic Medicine and ToxicologyNikhil K. MinaNo ratings yet
- Script - Un Chien AndalouDocument8 pagesScript - Un Chien AndalouSei-Kai LeungNo ratings yet
- Overpopulation in The Democratic Republic of The CongoDocument9 pagesOverpopulation in The Democratic Republic of The Congocheezpuff_1588210% (1)
- (Thomas Joiner) The Perversion of Virtue Understa PDFDocument266 pages(Thomas Joiner) The Perversion of Virtue Understa PDFA.VictorNo ratings yet
- Mitakuye OyasinDocument3 pagesMitakuye OyasinDel "Abe" JonesNo ratings yet
- H. S. Smith and D. G. Jeffreys - The Sacred Animal Necropolis, North Saqqara 1975-6, Vol - 63 (1977), Pp. 20-28 PDFDocument11 pagesH. S. Smith and D. G. Jeffreys - The Sacred Animal Necropolis, North Saqqara 1975-6, Vol - 63 (1977), Pp. 20-28 PDFnadaosmanNo ratings yet
- Asphyxia Causes, Sighn and SymtomDocument3 pagesAsphyxia Causes, Sighn and SymtomRian ArisyandiNo ratings yet
- WABForumSupplements SuccessorsDocument15 pagesWABForumSupplements SuccessorsskallabornNo ratings yet
- Pathology SWTDocument4 pagesPathology SWTkishorechandraNo ratings yet
- The Mahogany Table by Sylvia Townsend WarnerDocument3 pagesThe Mahogany Table by Sylvia Townsend WarnerRysal RuddinNo ratings yet
- Zelalem's Murder CaseDocument5 pagesZelalem's Murder CaseAnonymous vtg10A3TxdNo ratings yet
- ScopaDocument1 pageScopaThe Hamilton SpectatorNo ratings yet
- SH CP 146 Care of A Patient After Their Death Procedure V2 Jan 2017Document24 pagesSH CP 146 Care of A Patient After Their Death Procedure V2 Jan 2017malenatobeNo ratings yet
- Ovid's Metamorphoses: Pyramus & ThisbeDocument2 pagesOvid's Metamorphoses: Pyramus & Thisbeapi-262173560No ratings yet
- Mom SpellDocument48 pagesMom SpellFadzlli AminNo ratings yet
- The Poison Tree NotesDocument4 pagesThe Poison Tree Notesvolverin77836No ratings yet
- Mutation DescriptionsDocument34 pagesMutation DescriptionsBen SteigerNo ratings yet