You might also like
- DentistryDocument16 pagesDentistryMeka Syahputra56% (9)
- Printable Beers Pocket CardDocument4 pagesPrintable Beers Pocket CardJames Lindon100% (3)
- The DNA Way - Kashif KhanDocument268 pagesThe DNA Way - Kashif Khancepa100% (1)
- Acrrm Recalls Latest PDFDocument16 pagesAcrrm Recalls Latest PDFRumana Ali100% (2)
- Acog Practice Bulletin Summary: Gestational Hypertension and PreeclampsiaDocument4 pagesAcog Practice Bulletin Summary: Gestational Hypertension and PreeclampsiaKevin CasavilcaNo ratings yet
- National TB Control Program Form 7 - Referral FormDocument1 pageNational TB Control Program Form 7 - Referral FormAre Pee EtcNo ratings yet
- Postconcussion SyndromeDocument16 pagesPostconcussion SyndromeonaNo ratings yet
- Corona VirusesDocument42 pagesCorona VirusesSalah Elbadawy100% (5)
- Rhinovirus: Otitis Media and Sinusitis. ExacerbationsDocument34 pagesRhinovirus: Otitis Media and Sinusitis. ExacerbationsManisanthosh KumarNo ratings yet
- Corona ParamyxoviridaeDocument41 pagesCorona Paramyxoviridaeshikha yadavNo ratings yet
- Viruses of Relevance To Dentistry: Human PapillomavirusDocument6 pagesViruses of Relevance To Dentistry: Human Papillomavirusayman moaed alyasenNo ratings yet
- Respiratory Viruses: Coronaviruses, Influenza, Paramyxoviruses/TITLEDocument40 pagesRespiratory Viruses: Coronaviruses, Influenza, Paramyxoviruses/TITLEAsdfghjklNo ratings yet
- Respiratory Viral IllnessDocument43 pagesRespiratory Viral IllnessSiti TiaraNo ratings yet
- Viral Infections of The LRT: Dr. Muna M A Yousif MD Microbiology MSC Infection Control Frcpath Part 1Document27 pagesViral Infections of The LRT: Dr. Muna M A Yousif MD Microbiology MSC Infection Control Frcpath Part 1yasirNo ratings yet
- 05 PiconavirusDocument31 pages05 PiconavirusSAMMYNo ratings yet
- Negative Stranded RNA VirusesDocument47 pagesNegative Stranded RNA VirusesNovie Carla GayosaNo ratings yet
- Lec No (4) - Viral Respiratory Tract InfectionsDocument60 pagesLec No (4) - Viral Respiratory Tract InfectionsMohammedu IhthishamNo ratings yet
- Mycology IntroDocument8 pagesMycology IntroSagayduro Xyrille Angel N.No ratings yet
- Day 6 Virology - January 2021Document222 pagesDay 6 Virology - January 2021ShriefElghazalyNo ratings yet
- RNA Enveloped Viruses: Virus Family Medically Important VirusDocument19 pagesRNA Enveloped Viruses: Virus Family Medically Important VirusJaydee PlataNo ratings yet
- Enterovirus: Regati Meenakshi ROLL: B30Document27 pagesEnterovirus: Regati Meenakshi ROLL: B30Meena RajNo ratings yet
- Paramyxoviridae EditedDocument30 pagesParamyxoviridae EditedstudymedicNo ratings yet
- Adenoviruses AdenovirusesDocument25 pagesAdenoviruses AdenovirusesstudymedicNo ratings yet
- Viral Diseases of The Cardiovascular and Lympatic SystemDocument50 pagesViral Diseases of The Cardiovascular and Lympatic SystemHeuniceLoisSumabongNo ratings yet
- Corona VirusesDocument42 pagesCorona VirusesstudymedicNo ratings yet
- 58 - The Common Cold PDFDocument7 pages58 - The Common Cold PDFCarlos Urquijo100% (1)
- Viral Infection of The Respiratory SystemDocument18 pagesViral Infection of The Respiratory SystemAbdus SubhanNo ratings yet
- Myco Viro Hand Out Batch2 UpdatedDocument10 pagesMyco Viro Hand Out Batch2 UpdatedMark jay LlanoNo ratings yet
- Rubella: Prepared and Presented by Ibrahim Ali Assiri 439106123Document21 pagesRubella: Prepared and Presented by Ibrahim Ali Assiri 439106123عادل حكميNo ratings yet
- Common ColdDocument24 pagesCommon ColdAishwaryaNo ratings yet
- ParamyxovirusesDocument36 pagesParamyxovirusesRandy BerryNo ratings yet
- K.3 Pediatri-Virologi 3 2018-2019 PDFDocument76 pagesK.3 Pediatri-Virologi 3 2018-2019 PDFandi firdha restuwatiNo ratings yet
- Respiratory Infections 1Document62 pagesRespiratory Infections 1Eduardo Valdez RodríguezNo ratings yet
- Corona VirusesDocument61 pagesCorona VirusesNaing Lin SoeNo ratings yet
- Discovery of Influenza Virus: - First Isolated From A Pig in 1931 (Swine Flu) - Isolated From Human in 1933Document16 pagesDiscovery of Influenza Virus: - First Isolated From A Pig in 1931 (Swine Flu) - Isolated From Human in 1933api-19969058No ratings yet
- 5.1orthomyxoviridae 3Document23 pages5.1orthomyxoviridae 3Jiya MuhammadNo ratings yet
- Microbiology PathologyDocument114 pagesMicrobiology Pathologykhaleelkhamjan100% (1)
- SARS-2nd ProffDocument27 pagesSARS-2nd ProffMuhammad aslamNo ratings yet
- Viral Diseases 45Document27 pagesViral Diseases 45Mujtaba AlsalehNo ratings yet
- Microbiology FInal ReviewDocument4 pagesMicrobiology FInal ReviewAlexander PhamNo ratings yet
- Airborne and Direct Contact Viral Diseases: Transmission, Signs, and PreventionDocument97 pagesAirborne and Direct Contact Viral Diseases: Transmission, Signs, and PreventionAyushi AswalNo ratings yet
- RNA Viruses: Characteristics, Transmission, Diseases and Prevention of Major FamiliesDocument8 pagesRNA Viruses: Characteristics, Transmission, Diseases and Prevention of Major FamiliesBen SiradNo ratings yet
- MEASLES: SYMPTOMS, CAUSES, COMPLICATIONS AND PREVENTIONDocument34 pagesMEASLES: SYMPTOMS, CAUSES, COMPLICATIONS AND PREVENTIONmanibharathiNo ratings yet
- DR Channa Senanayake Dept of MicrobiologyDocument19 pagesDR Channa Senanayake Dept of MicrobiologyTharinduNo ratings yet
- Influenza VirusDocument28 pagesInfluenza VirusDave Despabiladeras100% (2)
- Wa0012. 1Document21 pagesWa0012. 1Sumita patelNo ratings yet
- Picornaviridae & Adenoviridae - Raja Pardomuan HarahapDocument63 pagesPicornaviridae & Adenoviridae - Raja Pardomuan HarahapM. RamazaliNo ratings yet
- Medicine Lec.9 - Viral Infection IIDocument42 pagesMedicine Lec.9 - Viral Infection II7fefdfbea1No ratings yet
- Infectious Diseases of The Respiratory SystemDocument51 pagesInfectious Diseases of The Respiratory SystemFachriza EffendiNo ratings yet
- Influenza, Pandemics and SARSDocument24 pagesInfluenza, Pandemics and SARSObatoye SeyiNo ratings yet
- Foundations in Microbiology: TalaroDocument76 pagesFoundations in Microbiology: Talaromertx013No ratings yet
- Acute Respiratory Viral Infections: Prof. S. M. Turyanitsa Dr. Karabinyosh S.ODocument29 pagesAcute Respiratory Viral Infections: Prof. S. M. Turyanitsa Dr. Karabinyosh S.ODOCTOR DanishNo ratings yet
- INFECTIONS OF THE RESPIRATORY TRACT AND G CompleteDocument39 pagesINFECTIONS OF THE RESPIRATORY TRACT AND G CompleteShekaina SumagangNo ratings yet
- ORTHOMYXOVIRUS and PARAMYXOVIRUSDocument21 pagesORTHOMYXOVIRUS and PARAMYXOVIRUSDaniel SantosNo ratings yet
- Chapter 9 Viral of Human DiseaseDocument6 pagesChapter 9 Viral of Human DiseaseMahrukh SaeedNo ratings yet
- Paramyxoviridae: For 3 Year MLS StudentsDocument57 pagesParamyxoviridae: For 3 Year MLS StudentsAbdurhman SeidNo ratings yet
- URTI (DR Hemin Khalid)Document21 pagesURTI (DR Hemin Khalid)Darawan MirzaNo ratings yet
- Chapter 2 - AiDocument37 pagesChapter 2 - AiHerjan SwandiNo ratings yet
- REOVIRUSESDocument28 pagesREOVIRUSESFrancis MakanyaNo ratings yet
- Aids 1Document31 pagesAids 1Angelica PantaleonNo ratings yet
- VIROLOGYDocument26 pagesVIROLOGYDickson MukunziNo ratings yet
- Chapter 13 Viral PathogenesisDocument68 pagesChapter 13 Viral PathogenesisKelly WareNo ratings yet
- Paramyxoviruses: Characteristics and Human PathogensDocument30 pagesParamyxoviruses: Characteristics and Human PathogensJaydee PlataNo ratings yet
- Respiratory PandemicsDocument5 pagesRespiratory PandemicsJiezl Abellano AfinidadNo ratings yet
- Micropara-1 Report:: Coronavirus 2019 Acute Respiratory DistressDocument32 pagesMicropara-1 Report:: Coronavirus 2019 Acute Respiratory DistressArlyn MarcelinoNo ratings yet
- Positive Stranded RNA VirusesDocument29 pagesPositive Stranded RNA VirusesNovie Carla GayosaNo ratings yet
- Heart FailureDocument7 pagesHeart FailurestudymedicNo ratings yet
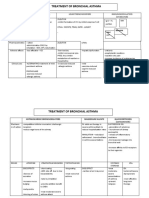
- Treatment of Bronchial AsthmaDocument3 pagesTreatment of Bronchial AsthmastudymedicNo ratings yet
- First Line Agents (Essentials) in Treatment of TBDocument2 pagesFirst Line Agents (Essentials) in Treatment of TBstudymedicNo ratings yet
- History Taking in Pulmonary MedicineDocument14 pagesHistory Taking in Pulmonary MedicinestudymedicNo ratings yet
- Introduction To Platyhelminthes (Flukes)Document78 pagesIntroduction To Platyhelminthes (Flukes)studymedicNo ratings yet
- Jugular VeinsDocument13 pagesJugular VeinsstudymedicNo ratings yet
- Symptoms of CvsDocument25 pagesSymptoms of CvsstudymedicNo ratings yet
- The Arterial PulseDocument22 pagesThe Arterial PulsestudymedicNo ratings yet
- Skills 2Document22 pagesSkills 2studymedicNo ratings yet
- Measles (Rubeola) VirusDocument16 pagesMeasles (Rubeola) Virusstudymedic100% (1)
- Inspection and Palpation of The HeartDocument38 pagesInspection and Palpation of The Heartstudymedic100% (2)
- General Examination For CVSDocument29 pagesGeneral Examination For CVSstudymedic100% (1)
- Blood PressureDocument11 pagesBlood PressurestudymedicNo ratings yet
- Pathology Practical Exam Study SheetDocument4 pagesPathology Practical Exam Study SheetstudymedicNo ratings yet
- Mumps VirusDocument15 pagesMumps Virusstudymedic0% (1)
- Paramyxoviridae EditedDocument30 pagesParamyxoviridae EditedstudymedicNo ratings yet
- Main Features of ParamyxovirusesDocument7 pagesMain Features of ParamyxovirusesstudymedicNo ratings yet
- Laboratory Diagnosis of Viral InfectionDocument37 pagesLaboratory Diagnosis of Viral InfectionstudymedicNo ratings yet
- Antihyperlipidaemic DrugsDocument44 pagesAntihyperlipidaemic DrugsstudymedicNo ratings yet
- Corona VirusesDocument42 pagesCorona VirusesstudymedicNo ratings yet
- Inspection and Palpation of The HeartDocument38 pagesInspection and Palpation of The Heartstudymedic100% (2)
- Adenoviruses AdenovirusesDocument25 pagesAdenoviruses AdenovirusesstudymedicNo ratings yet
- Practical Microbiology 2nd YearDocument33 pagesPractical Microbiology 2nd Yearstudymedic100% (1)
- Orthomyxoviruses Orthomyxoviruses Influenza Viruses Influenza VirusesDocument44 pagesOrthomyxoviruses Orthomyxoviruses Influenza Viruses Influenza VirusesstudymedicNo ratings yet
- Culture Media NoteDocument5 pagesCulture Media Notestudymedic100% (1)
- AllDocument54 pagesAlladham bani younesNo ratings yet
- IM Written Report Diabetes Case ReportDocument10 pagesIM Written Report Diabetes Case ReportJessa Mateum VallangcaNo ratings yet
- Vicente Sotto Memorial Medical CenterDocument17 pagesVicente Sotto Memorial Medical CenterNikki DiocampoNo ratings yet
- Living Things Other Than Plants and AnimalsDocument35 pagesLiving Things Other Than Plants and AnimalsClaudene GellaNo ratings yet
- Local anesthetic bupivacaine nursing considerationsDocument2 pagesLocal anesthetic bupivacaine nursing considerationsPutuNo ratings yet
- Wei PDFDocument12 pagesWei PDFVidyullathaa PrasadNo ratings yet
- Students With Mental RetardationDocument3 pagesStudents With Mental RetardationNorain KasanNo ratings yet
- Healing Wonders AppDocument18 pagesHealing Wonders AppJoanna Atrisk C-LealNo ratings yet
- Assessment of Using Guava Leaves As An Alternative Medicine For DiarrheaDocument32 pagesAssessment of Using Guava Leaves As An Alternative Medicine For DiarrheaKamela AliNo ratings yet
- Basic Geriatric Nursing 6th Edition Williams Test BankDocument10 pagesBasic Geriatric Nursing 6th Edition Williams Test Bankwheretoenough7rv77No ratings yet
- Constrictive PericarditisDocument54 pagesConstrictive PericarditisRazib AlamNo ratings yet
- Hospital Diet GuideDocument6 pagesHospital Diet GuidejhelabooNo ratings yet
- Ii Anatomy+and+physiologyDocument2 pagesIi Anatomy+and+physiologybillyktoubattsNo ratings yet
- FM Shelf Exam ReviewDocument5 pagesFM Shelf Exam ReviewMohammad Katato100% (1)
- 25 UrologyDocument47 pages25 UrologyMahmoud AbuAwadNo ratings yet
- Disorders of Endocrine GlandDocument14 pagesDisorders of Endocrine Glandaklimaetsy1099No ratings yet
- Curriculum Map in Mapeh 8 (Quarter 3)Document17 pagesCurriculum Map in Mapeh 8 (Quarter 3)Lucelyn Lugas CapoyNo ratings yet
- A Topic Presentation ON: Emerging Communicable DiseasesDocument52 pagesA Topic Presentation ON: Emerging Communicable DiseasesGiri SivaNo ratings yet
- Briefing Practical Literature Searching and Critical Appraisal (Diagnosis and Therapy) - Dr. Lukman Ade Chandra, M.med., M. Phil (2022)Document16 pagesBriefing Practical Literature Searching and Critical Appraisal (Diagnosis and Therapy) - Dr. Lukman Ade Chandra, M.med., M. Phil (2022)Sheila Tirta AyumurtiNo ratings yet
- A Balanced Diet Is One That Provides An Adequate Intake of Energy and Nutrients For Maintenance of The Body and Therefore Good HealthDocument1 pageA Balanced Diet Is One That Provides An Adequate Intake of Energy and Nutrients For Maintenance of The Body and Therefore Good HealthSnigdha SarkarNo ratings yet
- History TakingDocument13 pagesHistory TakingSirajum MuneeraNo ratings yet
- Social Anxiety Disorder 1.editedDocument4 pagesSocial Anxiety Disorder 1.editedmoureenNo ratings yet
- Heart PathologyDocument8 pagesHeart PathologyJose SirittNo ratings yet