You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Life in The Ancient WorldDocument48 pagesLife in The Ancient Worldjmagil6092100% (1)
- Rockwell Collins RDRDocument24 pagesRockwell Collins RDRMatty Torchia100% (5)
- Ed Post Lab Heat of Formation of NaClDocument4 pagesEd Post Lab Heat of Formation of NaClEdimar ManlangitNo ratings yet
- Better Photography - April 2018 PDFDocument100 pagesBetter Photography - April 2018 PDFPeter100% (1)
- Ch06 Allocating Resources To The ProjectDocument55 pagesCh06 Allocating Resources To The ProjectJosh ChamaNo ratings yet
- Tetra IntroductionDocument65 pagesTetra Introductionuniversidaddistrital100% (2)
- Pricing of A Revolutionary ProductDocument22 pagesPricing of A Revolutionary ProductiluvparixitNo ratings yet
- Neelima A Kulkarni ResumeDocument3 pagesNeelima A Kulkarni ResumeAcademics LecturenotesNo ratings yet
- Model TB-16Document20 pagesModel TB-16xuanphuong2710No ratings yet
- Pt. Trijaya Agro FoodsDocument18 pagesPt. Trijaya Agro FoodsJie MaNo ratings yet
- Report On Marketing Strategy of Nestle MILKPAKDocument13 pagesReport On Marketing Strategy of Nestle MILKPAKAzeem Ahmad100% (1)
- Geometry and IntuitionDocument9 pagesGeometry and IntuitionHollyNo ratings yet
- Dialog InggrisDocument4 pagesDialog Inggrisبايو سيتياوانNo ratings yet
- Docsity Detailed Lesson Plan 5Document4 pagesDocsity Detailed Lesson Plan 5Sydie MoredoNo ratings yet
- Laboratorio 1Document6 pagesLaboratorio 1Marlon DiazNo ratings yet
- Hetal Patel: Team Leader - SalesDocument2 pagesHetal Patel: Team Leader - SalesPrashant kumarNo ratings yet
- Taylor Et Al v. Acxiom Corporation Et Al - Document No. 91Document40 pagesTaylor Et Al v. Acxiom Corporation Et Al - Document No. 91Justia.comNo ratings yet
- College of Computer Science Software DepartmentDocument4 pagesCollege of Computer Science Software DepartmentRommel L. DorinNo ratings yet
- LS01 ServiceDocument53 pagesLS01 ServicehutandreiNo ratings yet
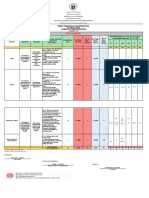
- Revised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10Document6 pagesRevised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10May Ann GuintoNo ratings yet
- Bigbazaar PDFDocument14 pagesBigbazaar PDFazhagu sundaramNo ratings yet
- CoSiO2 For Fischer-Tropsch Synthesis Comparison...Document5 pagesCoSiO2 For Fischer-Tropsch Synthesis Comparison...Genesis CalderónNo ratings yet
- Ae - Centuries Before 1400 Are Listed As Browsable DirectoriesDocument3 pagesAe - Centuries Before 1400 Are Listed As Browsable DirectoriesPolNeimanNo ratings yet
- Restaurant Report Card: February 9, 2023Document4 pagesRestaurant Report Card: February 9, 2023KBTXNo ratings yet
- Explore The WorldDocument164 pagesExplore The WorldEduardo C VanciNo ratings yet
- Kidney Stone Diet 508Document8 pagesKidney Stone Diet 508aprilNo ratings yet
- IG Deck Seal PumpDocument3 pagesIG Deck Seal PumpSergei KurpishNo ratings yet
- Code ExplanantionDocument4 pagesCode ExplanantionVivek JadiyaNo ratings yet
- Research On Export Trade in BangladeshDocument7 pagesResearch On Export Trade in BangladeshFarjana AnwarNo ratings yet
- M.Plan SYLLABUS 2022-24Document54 pagesM.Plan SYLLABUS 2022-24Mili DawsonNo ratings yet