You might also like
- Surat Izin Instansi TKHIDocument1 pageSurat Izin Instansi TKHILianSiahaanNo ratings yet
- A Randomized Trial of Icatibant in ACE-Inhibitor-Induced AngioedemaDocument8 pagesA Randomized Trial of Icatibant in ACE-Inhibitor-Induced AngioedemaEmy Noviana SandyNo ratings yet
- Lembar Follow Up SarafDocument1 pageLembar Follow Up SarafLianSiahaanNo ratings yet
- Kuliah Anatomi Fisiologi DR - BramDocument60 pagesKuliah Anatomi Fisiologi DR - BramLianSiahaanNo ratings yet
- Handbook Utk S1 PDFDocument21 pagesHandbook Utk S1 PDFatikaNo ratings yet
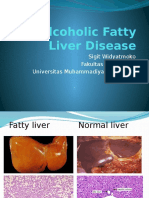
- Fatty LiverDocument31 pagesFatty LiverLianSiahaanNo ratings yet
- Nej Mo A 1609214Document7 pagesNej Mo A 1609214LianSiahaanNo ratings yet
- A Randomized Trial of Low-Cost Mesh in Groin Hernia Repair: Original ArticleDocument8 pagesA Randomized Trial of Low-Cost Mesh in Groin Hernia Repair: Original ArticleLianSiahaanNo ratings yet
- Alternatif Terapi, Pelengkap, Dan Pengobatan Terlupakan Dermatitis AtopiDocument11 pagesAlternatif Terapi, Pelengkap, Dan Pengobatan Terlupakan Dermatitis AtopiLianSiahaanNo ratings yet
- 37 FullDocument3 pages37 FullLianSiahaanNo ratings yet
- A Deadly Chip Was Implanted in His Brain by Evil AliensDocument1 pageA Deadly Chip Was Implanted in His Brain by Evil AliensLianSiahaanNo ratings yet
- HistologiDocument1 pageHistologiLianSiahaanNo ratings yet
- Blok THT 1Document6 pagesBlok THT 1LianSiahaanNo ratings yet
- Anatomy & Physiology of Lacrimal Secretion & Outflow: DR - Nurcahya Ab, SPMDocument51 pagesAnatomy & Physiology of Lacrimal Secretion & Outflow: DR - Nurcahya Ab, SPMLianSiahaanNo ratings yet
- Pendukung Jurnal DiabetesDocument32 pagesPendukung Jurnal DiabetesLianSiahaanNo ratings yet
- Gambar Skenario Minggu Pertama Blok SkinDocument1 pageGambar Skenario Minggu Pertama Blok SkinLianSiahaanNo ratings yet
- Wohlegemuth Albumin BANG Percobaa Proteinuri 1Document2 pagesWohlegemuth Albumin BANG Percobaa Proteinuri 1LianSiahaanNo ratings yet
- Tumor With The Features of Both Squamous Cell Carcinoma and Melanoma (Melanocarcinoma)Document3 pagesTumor With The Features of Both Squamous Cell Carcinoma and Melanoma (Melanocarcinoma)LianSiahaanNo ratings yet
- Wohlegemuth Albumin BANG Percobaa Proteinuri 1Document2 pagesWohlegemuth Albumin BANG Percobaa Proteinuri 1LianSiahaanNo ratings yet
- MesotheliomaDocument46 pagesMesotheliomaLianSiahaanNo ratings yet
- Gambaran Rad Musc Abnormal, FK UMS, 2014Document120 pagesGambaran Rad Musc Abnormal, FK UMS, 2014LianSiahaanNo ratings yet
- Krisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranDocument67 pagesKrisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranLianSiahaanNo ratings yet
- A Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarDocument9 pagesA Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarLianSiahaanNo ratings yet
- Guideline Heart FailureDocument34 pagesGuideline Heart FailureLianSiahaanNo ratings yet
- AaaDocument7 pagesAaaLianSiahaanNo ratings yet
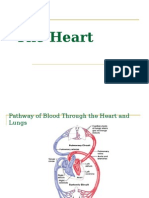
- HeartDocument45 pagesHeartamelialyNo ratings yet
- New Strategi Diagnosis An-Intern 09Document71 pagesNew Strategi Diagnosis An-Intern 09LianSiahaanNo ratings yet
- ITS Undergraduate 17368 BibliographyDocument4 pagesITS Undergraduate 17368 BibliographyLianSiahaanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Diabetes - Full PageDocument64 pagesDiabetes - Full PagerasmeetNo ratings yet
- CPG Management of Type 2 Diabetes Mellitus (4th Edition)Document84 pagesCPG Management of Type 2 Diabetes Mellitus (4th Edition)apalaginih100% (3)
- A Study To Assess The Effectiveness of Fenugreek Water To Reduce Blood Glucose Levels Among Clients With Diabetes MellitusDocument5 pagesA Study To Assess The Effectiveness of Fenugreek Water To Reduce Blood Glucose Levels Among Clients With Diabetes MellitusEditor IJTSRDNo ratings yet
- Unit 7 Diabetes Student ResourcesDocument7 pagesUnit 7 Diabetes Student ResourcesScribdNo ratings yet
- Diabetes QuestionsDocument8 pagesDiabetes QuestionsJohn Osborne100% (1)
- Ajcpath112 0665Document10 pagesAjcpath112 0665RiyanNo ratings yet
- IDF Diabetes Atlas: Global Estimates of Undiagnosed Diabetes in Adults For 2021Document9 pagesIDF Diabetes Atlas: Global Estimates of Undiagnosed Diabetes in Adults For 2021Usee TvNo ratings yet
- The Effects of Lifestyle For The Management of Patient With Diabetes Mellitus Type 2Document33 pagesThe Effects of Lifestyle For The Management of Patient With Diabetes Mellitus Type 2EduNo ratings yet
- Diabetes and Ocular Disease PDFDocument513 pagesDiabetes and Ocular Disease PDFmdmmm100% (1)
- Group H (Sn.8) Lab ReportDocument152 pagesGroup H (Sn.8) Lab ReportNishrita DevnathNo ratings yet
- International Journal of Diabetes and Clinical Research Ijdcr 7 128Document7 pagesInternational Journal of Diabetes and Clinical Research Ijdcr 7 128Yaseen MohamnadNo ratings yet
- Blood tests help diagnose diseasesDocument10 pagesBlood tests help diagnose diseasesMay Mawzi WahabNo ratings yet
- Aace/Ace Comprehensive Type 2 Diabetes Management Algorithm: Sherwin D'Souza, MD, FACEDocument30 pagesAace/Ace Comprehensive Type 2 Diabetes Management Algorithm: Sherwin D'Souza, MD, FACEKok Hui DiongNo ratings yet
- ResearchDocument112 pagesResearchavnishNo ratings yet
- Bihag Quiz Medicine AreaDocument5 pagesBihag Quiz Medicine AreaDan HizonNo ratings yet
- Diabetes - Frequently Asked QuestionsDocument6 pagesDiabetes - Frequently Asked QuestionsAnish GobyNo ratings yet
- Somatropin For Injection I.P. (r-DNA Origin) : HumatropeDocument2 pagesSomatropin For Injection I.P. (r-DNA Origin) : HumatropeAdityaraj SinhaNo ratings yet
- Diabetes, Often Referred To by Doctors As Diabetes Mellitus, Describes A Group of MetabolicDocument4 pagesDiabetes, Often Referred To by Doctors As Diabetes Mellitus, Describes A Group of MetabolicLheiDanielMariellMonteroNo ratings yet
- Proposal Abdu SelamDocument18 pagesProposal Abdu SelamAbdulaziz TilahunNo ratings yet
- DM Type 2Document153 pagesDM Type 2Taufiqurrochman Nur AminNo ratings yet
- Slide Rehab MedikDocument18 pagesSlide Rehab MedikElfan Mahfuzh SmavenNo ratings yet
- ADA 2014 - Standards of Medical Care in DiabetesDocument67 pagesADA 2014 - Standards of Medical Care in Diabetesjack jackNo ratings yet
- DAIBETESDocument23 pagesDAIBETESAditya MahakalNo ratings yet
- Synergy Science: The Benefits of Echo WaterDocument9 pagesSynergy Science: The Benefits of Echo WaterSubbaraju GvNo ratings yet
- Research Paper 1Document5 pagesResearch Paper 1api-315856517No ratings yet
- Biomarkers of AgingDocument12 pagesBiomarkers of AgingLjón BjörnNo ratings yet
- FULL Guideline SOGC 2005 2016Document756 pagesFULL Guideline SOGC 2005 2016dr.razi100% (1)
- Nurs Fpx 4030 Assessment 3 Pico t Questions and an Evidence Based ApproachDocument6 pagesNurs Fpx 4030 Assessment 3 Pico t Questions and an Evidence Based Approachzadem5266No ratings yet
- Case Study On: Lyceum of The Philippines UniversityDocument4 pagesCase Study On: Lyceum of The Philippines UniversityarturogarcesjrNo ratings yet
- Presentation Diagnosis of Diabetes Mellitus: Presented by Kanwal AmjadDocument29 pagesPresentation Diagnosis of Diabetes Mellitus: Presented by Kanwal AmjadSpencerNo ratings yet