You might also like
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Primary Adrenal InsufficiencyDocument26 pagesPrimary Adrenal InsufficiencyEmily EresumaNo ratings yet
- More Than A Sore ThroatDocument17 pagesMore Than A Sore ThroatEmily EresumaNo ratings yet
- MysteryCase 10.22.18Document10 pagesMysteryCase 10.22.18Emily EresumaNo ratings yet
- Morning Report: August 28, 2013 Jessica Miller, MD, PGY2Document30 pagesMorning Report: August 28, 2013 Jessica Miller, MD, PGY2Emily EresumaNo ratings yet
- Bells Palsy or Stroke 02.06.2019Document19 pagesBells Palsy or Stroke 02.06.2019Emily EresumaNo ratings yet
- Practice Based Learning (Grand Round)Document48 pagesPractice Based Learning (Grand Round)AnnumNo ratings yet
- Botulism 08.16.2013Document12 pagesBotulism 08.16.2013Emily EresumaNo ratings yet
- Limping 12.10.2018Document32 pagesLimping 12.10.2018Emily Eresuma100% (1)
- Morning Report 9/5/18: Adam Cardullo, MD Pgy - 2Document22 pagesMorning Report 9/5/18: Adam Cardullo, MD Pgy - 2Emily EresumaNo ratings yet
- Pediatric Urology Topics Relating To Infants & Toddlers: Danielle Brady, Pgy-2Document35 pagesPediatric Urology Topics Relating To Infants & Toddlers: Danielle Brady, Pgy-2Emily EresumaNo ratings yet
- Zebras of Neonatal Hypoglycemia 06.09.2014Document21 pagesZebras of Neonatal Hypoglycemia 06.09.2014Emily EresumaNo ratings yet
- TularemiaDocument19 pagesTularemiaEmily EresumaNo ratings yet
- Cyclic VomitingDocument19 pagesCyclic VomitingEmily EresumaNo ratings yet
- Short StatureDocument14 pagesShort StatureEmily EresumaNo ratings yet
- Morning Report: Sarah Todd, PGY-3 August 7, 2015Document19 pagesMorning Report: Sarah Todd, PGY-3 August 7, 2015Emily EresumaNo ratings yet
- POLYCYTHEMIADocument29 pagesPOLYCYTHEMIAFaizan KhanNo ratings yet
- Jeffrey Barratt, MDDocument27 pagesJeffrey Barratt, MDEmily EresumaNo ratings yet
- Clinico-Pathologic Conference 2015Document43 pagesClinico-Pathologic Conference 2015Ezekiel ArtetaNo ratings yet
- Pediatrics Osce: Done By: Mohammed I. Alhefzi. Othman M. Omair Dec. 2011Document71 pagesPediatrics Osce: Done By: Mohammed I. Alhefzi. Othman M. Omair Dec. 2011marina_shawkyNo ratings yet
- Approach To Hematuria and Proteinuria in ChildrenDocument52 pagesApproach To Hematuria and Proteinuria in ChildrenMysheb SS100% (1)
- FTT Causes, Symptoms & TreatmentDocument15 pagesFTT Causes, Symptoms & TreatmentSiti Nursuhada binti Mohd AminNo ratings yet
- Sickle Cell Anemia PowerpointDocument29 pagesSickle Cell Anemia Powerpointapi-263353704100% (1)
- Hypocalcemia: Dr. Nicolette Du Plessis Department PaediatricsDocument40 pagesHypocalcemia: Dr. Nicolette Du Plessis Department PaediatricsBharath Reddy DNo ratings yet
- Clinicopathological Conference 2Document23 pagesClinicopathological Conference 2Rem AlfelorNo ratings yet
- 24 HR History 2Document2 pages24 HR History 2Arjun KatariaNo ratings yet
- Abdominal Pain in ChildrenDocument48 pagesAbdominal Pain in ChildrenSurin Jayawardene100% (1)
- EnuresisDocument31 pagesEnuresisEmily EresumaNo ratings yet
- Board Prep Metabolics Feb 2019Document23 pagesBoard Prep Metabolics Feb 2019Emily EresumaNo ratings yet
- GROUP 3 Case PresentationDocument35 pagesGROUP 3 Case PresentationDinesh KumarNo ratings yet
- Oral Cases Study Guide - PediatricsDocument68 pagesOral Cases Study Guide - PediatricsJohn100% (1)
- Cow's Milk Protein AllergyDocument46 pagesCow's Milk Protein AllergyChyntia PutriNo ratings yet
- Common Newborn Problems (2) C1Document39 pagesCommon Newborn Problems (2) C1ZmNo ratings yet
- Final GIT Case PresentationDocument53 pagesFinal GIT Case PresentationRovan100% (1)
- Morning Report: Jawaria K. Alam, MD/PGY3Document20 pagesMorning Report: Jawaria K. Alam, MD/PGY3Emily EresumaNo ratings yet
- SOAP Note 1Document4 pagesSOAP Note 1AdamNo ratings yet
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56No ratings yet
- Panpacific University Nursing Students Report on Acute Gastroenteritis CaseDocument20 pagesPanpacific University Nursing Students Report on Acute Gastroenteritis CaseMar OrdanzaNo ratings yet
- Pediatric Department Faculty of MedicineDocument100 pagesPediatric Department Faculty of MedicineIrfanNo ratings yet
- Somatization 01.28.2019Document28 pagesSomatization 01.28.2019Emily EresumaNo ratings yet
- Facial Edema and Kidney Disease in a 5-Year-Old BoyDocument13 pagesFacial Edema and Kidney Disease in a 5-Year-Old BoyLuigi FranciscoNo ratings yet
- Failure To Thrive: Premi Suresh, MD, FAAPDocument57 pagesFailure To Thrive: Premi Suresh, MD, FAAPsiti hazard aldinaNo ratings yet
- PedsCases - Anaphylaxis Emergency TreatmentDocument5 pagesPedsCases - Anaphylaxis Emergency TreatmentSara Ilyas KhanNo ratings yet
- A Placebo-Controlled Trial of Silymarin in Patients With Nonalcoholic Fatty Liver DiseaseDocument6 pagesA Placebo-Controlled Trial of Silymarin in Patients With Nonalcoholic Fatty Liver Diseasesnn123456No ratings yet
- MRCPCH Part Ii: Safdar Iqbal'sDocument5 pagesMRCPCH Part Ii: Safdar Iqbal'sGalaleldin AliNo ratings yet
- Abdominal Pain Guide for Diagnosis and Treatment (39Document23 pagesAbdominal Pain Guide for Diagnosis and Treatment (39C Dimacali100% (1)
- Cyanotic Congenital Heart DiseaseDocument22 pagesCyanotic Congenital Heart DiseaseRaviNo ratings yet
- Infant and Young Child Feeding: Dr. Malik Shahnawaz AhmedDocument71 pagesInfant and Young Child Feeding: Dr. Malik Shahnawaz AhmedRiyaz AhamedNo ratings yet
- Newborn NotesDocument44 pagesNewborn NotesHaziq KamardinNo ratings yet
- Masalah Gastrointestinal KolestasisDocument21 pagesMasalah Gastrointestinal KolestasisMuthi'ah Ramadhani AgusNo ratings yet
- Picu Case StudyDocument3 pagesPicu Case Studyapi-455545776No ratings yet
- Nephrotic Syndrome and Glomerulonephritis GuideDocument40 pagesNephrotic Syndrome and Glomerulonephritis GuidesangheetaNo ratings yet
- Depression in AdolescentDocument13 pagesDepression in AdolescentSusan KoshyNo ratings yet
- Clinical Case: Section A - Group 8Document68 pagesClinical Case: Section A - Group 8madison Deli100% (1)
- VPD RashchrtDocument2 pagesVPD RashchrtMarco Ramos JacobNo ratings yet
- K21-Fever With RashDocument76 pagesK21-Fever With RashMarisa Perucana SinambelaNo ratings yet
- RNSG 1533 Raising The Bar For Success Concept: Metabolism: Diabetes Type 1/diabetes Type 2Document4 pagesRNSG 1533 Raising The Bar For Success Concept: Metabolism: Diabetes Type 1/diabetes Type 2katrinasdNo ratings yet
- Celiac Disease in ChildrenDocument59 pagesCeliac Disease in Childrend-fbuser-57045067No ratings yet
- Nausea VomitingDocument36 pagesNausea VomitingDian Fitri100% (1)
- Neonatal Hepatitis SyndromeDocument18 pagesNeonatal Hepatitis Syndromeenny_rommyNo ratings yet
- Morning Report Case Presentation: APRIL 1, 2019Document14 pagesMorning Report Case Presentation: APRIL 1, 2019Emily EresumaNo ratings yet
- Kidney Disorders 03.27.2019Document33 pagesKidney Disorders 03.27.2019Emily EresumaNo ratings yet
- Investing 101 For Residents: RJ Nemeyer MDDocument12 pagesInvesting 101 For Residents: RJ Nemeyer MDEmily EresumaNo ratings yet
- Case Presentation: Tad MiyaDocument41 pagesCase Presentation: Tad MiyaEmily EresumaNo ratings yet
- Board Prep Metabolics Feb 2019Document23 pagesBoard Prep Metabolics Feb 2019Emily EresumaNo ratings yet
- Board Prep Genetics Dec 2018Document62 pagesBoard Prep Genetics Dec 2018Emily EresumaNo ratings yet
- Dangers of Vaping 03.15.2019Document23 pagesDangers of Vaping 03.15.2019Emily EresumaNo ratings yet
- Pediatric Hypertension Noon Conference 03.20.2019Document44 pagesPediatric Hypertension Noon Conference 03.20.2019Emily EresumaNo ratings yet
- Food Challenge 03.20.2019Document17 pagesFood Challenge 03.20.2019Emily EresumaNo ratings yet
- Ophtho Pearls 03.13.2019Document17 pagesOphtho Pearls 03.13.2019Emily EresumaNo ratings yet
- Tachycardia How To Keep Your Patient Alive in The Middle of The NightDocument30 pagesTachycardia How To Keep Your Patient Alive in The Middle of The NightEmily Eresuma100% (1)
- Chronic Granulomatous Disease 01.23.2019Document10 pagesChronic Granulomatous Disease 01.23.2019Emily EresumaNo ratings yet
- Somatization 01.28.2019Document28 pagesSomatization 01.28.2019Emily EresumaNo ratings yet
- Anemia: Erika Franz-O'Neal PGY-2 Pediatric ResidentDocument16 pagesAnemia: Erika Franz-O'Neal PGY-2 Pediatric ResidentEmily EresumaNo ratings yet
- Pertussis 01.14.2019Document29 pagesPertussis 01.14.2019Emily EresumaNo ratings yet
- Morning Report: JANUARY 7, 2019 Katie Mailey, Pgy2Document24 pagesMorning Report: JANUARY 7, 2019 Katie Mailey, Pgy2Emily EresumaNo ratings yet
- Board Prep GI Jan 2019Document32 pagesBoard Prep GI Jan 2019Emily EresumaNo ratings yet
- Morning Report: Melanie Nelson, PGY-2Document25 pagesMorning Report: Melanie Nelson, PGY-2Emily EresumaNo ratings yet
- Limping 12.10.2018Document32 pagesLimping 12.10.2018Emily Eresuma100% (1)
- Ventilators 11.07.2018Document38 pagesVentilators 11.07.2018Emily EresumaNo ratings yet
- Board Prep Emergency Ingestions Dec.2018Document46 pagesBoard Prep Emergency Ingestions Dec.2018Emily EresumaNo ratings yet
- Morning Report: Lindsey Gakenheimer-Smith MD PGY3Document20 pagesMorning Report: Lindsey Gakenheimer-Smith MD PGY3Emily EresumaNo ratings yet
- Wilderness Medicine 11.20.2018Document12 pagesWilderness Medicine 11.20.2018Emily EresumaNo ratings yet
- Pediatric Urology Topics Relating To Infants & Toddlers: Danielle Brady, Pgy-2Document35 pagesPediatric Urology Topics Relating To Infants & Toddlers: Danielle Brady, Pgy-2Emily EresumaNo ratings yet
- Morning Report: Wade Harrison, MD, MPHDocument13 pagesMorning Report: Wade Harrison, MD, MPHEmily EresumaNo ratings yet
- Jaundice 11.28.2018Document13 pagesJaundice 11.28.2018Emily EresumaNo ratings yet
- Halloween Safety: Dominique ChevalierDocument21 pagesHalloween Safety: Dominique ChevalierEmily EresumaNo ratings yet
- Foster Care in Utah: Marlayna DespresDocument11 pagesFoster Care in Utah: Marlayna DespresEmily EresumaNo ratings yet
- Appendix L HHRA CombinedDocument428 pagesAppendix L HHRA Combinedwholmes5924No ratings yet
- Posted: Mon Jun 21, 2010 4:02 PM Post Subject: DENTAL MCQS: Previous Year PaperDocument16 pagesPosted: Mon Jun 21, 2010 4:02 PM Post Subject: DENTAL MCQS: Previous Year PaperMadhul Singhal100% (1)
- LymphomaDocument13 pagesLymphomaRAJKUMARNo ratings yet
- Kenya Medical Training College - Nyamira End of Year Three Semester One Examination March 2015 KRCHN Class (Pre-Service)Document4 pagesKenya Medical Training College - Nyamira End of Year Three Semester One Examination March 2015 KRCHN Class (Pre-Service)Mursal RashidNo ratings yet
- CCRN-PCCN Review RenalDocument11 pagesCCRN-PCCN Review RenalGiovanni MictilNo ratings yet
- Emergency Surgery Section ECTES 2018 ValenciaDocument5 pagesEmergency Surgery Section ECTES 2018 Valenciagarbass1905No ratings yet
- The New Version 9 American Joint Committee On CancDocument12 pagesThe New Version 9 American Joint Committee On CancardiNo ratings yet
- NBME 2 Block 1-4 EditedDocument88 pagesNBME 2 Block 1-4 EditedMayank Gogna100% (2)
- Unit 830 Level 3 Monitor and Maintain Spa Area Treatment Evidence FormDocument3 pagesUnit 830 Level 3 Monitor and Maintain Spa Area Treatment Evidence FormJowie SooNo ratings yet
- An Unusual Location of Carcinoma: The Clitoris and The VulvaDocument2 pagesAn Unusual Location of Carcinoma: The Clitoris and The VulvaIOSRjournalNo ratings yet
- Science of The Total EnvironmentDocument11 pagesScience of The Total EnvironmentUsman AliNo ratings yet
- Dr. Nugroho Sigit SpRad PDFDocument20 pagesDr. Nugroho Sigit SpRad PDFMira HandayaniNo ratings yet
- Board Notes and QuestionsDocument481 pagesBoard Notes and QuestionsAnil S. BhavsarNo ratings yet
- CeramFab Inc. & WYG Refractories SuitDocument27 pagesCeramFab Inc. & WYG Refractories SuitBenjamin DuerNo ratings yet
- Concept Map 5Document2 pagesConcept Map 5api-354331689No ratings yet
- Step 2 CK QuestionsDocument8 pagesStep 2 CK QuestionsIrfan Majeed50% (2)
- Lead-Acid Battery Safety Data SheetDocument4 pagesLead-Acid Battery Safety Data SheetosuwiraNo ratings yet
- Zikes - Jaaha - 2012 - Bilateral Ventriculocordectomy Via Ventral Approach For LAR PARDocument11 pagesZikes - Jaaha - 2012 - Bilateral Ventriculocordectomy Via Ventral Approach For LAR PARranderson1972No ratings yet
- Celiac DiseaseDocument42 pagesCeliac DiseaseTri P BukerNo ratings yet
- Kjjhhgfdsasdf HJKLKJHGFDSSDFG HJKLDocument4 pagesKjjhhgfdsasdf HJKLKJHGFDSSDFG HJKLbubble_inNo ratings yet
- RESEARCH PROPOSAL - 3 Nov 2013 PDFDocument27 pagesRESEARCH PROPOSAL - 3 Nov 2013 PDFWestley AbluyenNo ratings yet
- Mov3. GENERAL - UMN (Pyramidal) & LMN DisordersDocument9 pagesMov3. GENERAL - UMN (Pyramidal) & LMN DisordersherlambangkusumoNo ratings yet
- Newly Diagnosed GlioblastomaDocument30 pagesNewly Diagnosed GlioblastomaJubairNo ratings yet
- Adult T-Cell Leukemia Lymphoma (Atll) A Rare Case Associated With Human T-Cell Virus (Htlv-1)Document19 pagesAdult T-Cell Leukemia Lymphoma (Atll) A Rare Case Associated With Human T-Cell Virus (Htlv-1)Priya ChandakNo ratings yet
- مجلة توفيقTJMSDocument89 pagesمجلة توفيقTJMSTaghreed Hashim al-NoorNo ratings yet
- BRS General Surgery-1 PDFDocument117 pagesBRS General Surgery-1 PDFShermalyn Riva Hamid100% (2)
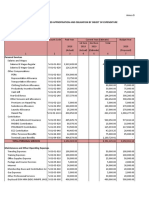
- Programmed Appropriation and Obligation by Object of ExpenditureDocument7 pagesProgrammed Appropriation and Obligation by Object of ExpenditureKristin Villaseñor-MercadoNo ratings yet
- Thrombo PhiliaDocument226 pagesThrombo PhiliawalkerbestNo ratings yet
- Causes and Indications in OphthalmologyDocument46 pagesCauses and Indications in Ophthalmologymarina_shawkyNo ratings yet
- Clinical Study Baccharis Dracunculifolia As Agent For The Control of BiofilmDocument7 pagesClinical Study Baccharis Dracunculifolia As Agent For The Control of BiofilmimamaptNo ratings yet