You might also like
- Brucelosis en niños: causas, síntomas y tratamientoDocument17 pagesBrucelosis en niños: causas, síntomas y tratamientoEda DonayreNo ratings yet
- La Amà GdalaDocument20 pagesLa Amà GdalaEda DonayreNo ratings yet
- Abscesos cerebrales múltiples micóticos en paciente inmunocompetenteDocument2 pagesAbscesos cerebrales múltiples micóticos en paciente inmunocompetenteEda DonayreNo ratings yet
- Lóbulo FrontalDocument14 pagesLóbulo FrontalEda DonayreNo ratings yet
- Eda Donayre Rodríguez HamaDocument62 pagesEda Donayre Rodríguez HamaEda DonayreNo ratings yet
- Desarrollo Del Ojo y Agudeza VisualDocument56 pagesDesarrollo Del Ojo y Agudeza VisualEda DonayreNo ratings yet
- CISTICERCOSIS 2015 UsjbDocument22 pagesCISTICERCOSIS 2015 UsjbEda DonayreNo ratings yet
- CoquelucheDocument61 pagesCoquelucheEda DonayreNo ratings yet
- 1INTUBACIONDocument1 page1INTUBACIONEda DonayreNo ratings yet
- Miliaria Tiña CapitisDocument56 pagesMiliaria Tiña CapitisEda Donayre100% (1)
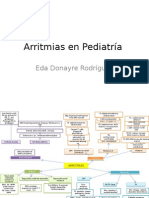
- ArritmiasDocument3 pagesArritmiasEda DonayreNo ratings yet
- Uso Racional de ATB: Eda Donayre RodríguezDocument4 pagesUso Racional de ATB: Eda Donayre RodríguezEda DonayreNo ratings yet
- TBC Expo MadridDocument109 pagesTBC Expo MadridEda DonayreNo ratings yet
- Diabetes Tipo IDocument24 pagesDiabetes Tipo IEda DonayreNo ratings yet
- Triaje y Admision A Sala de Observacion Pediatric A Vers. 2007Document49 pagesTriaje y Admision A Sala de Observacion Pediatric A Vers. 2007Eda DonayreNo ratings yet
- ANAFILAXIADocument30 pagesANAFILAXIAEda DonayreNo ratings yet
- Adoum Jorge Rasgando VelosDocument80 pagesAdoum Jorge Rasgando VelosMAIKHOL4100% (1)
- Microbiologia de La CarneDocument19 pagesMicrobiologia de La CarneIsidoro Neyra CamposNo ratings yet
- Valores Normales en PediatriaDocument8 pagesValores Normales en PediatriahelesarNo ratings yet
- Cuadro ComparativoDocument10 pagesCuadro ComparativoGinellie Lopez GongoraNo ratings yet
- La mujer que mató a los pecesDocument17 pagesLa mujer que mató a los pecesJo Aqu ÍnNo ratings yet
- Guía de Histología del Sistema RespiratorioDocument7 pagesGuía de Histología del Sistema RespiratorioJuan Pimiento PerezNo ratings yet
- Absceso PulmonarDocument29 pagesAbsceso PulmonarIvan Yamil Medina CarrilloNo ratings yet
- Triásico período geológicoDocument12 pagesTriásico período geológicoAngel l y 18No ratings yet
- Resumen Introducción Sistema EsqueléticoDocument3 pagesResumen Introducción Sistema EsqueléticoShmuel Ben ELOHIMNo ratings yet
- Hemoglobina y MioglobinaDocument12 pagesHemoglobina y MioglobinarodivaxNo ratings yet
- Exámenes de HematologíaDocument28 pagesExámenes de HematologíaSheryl BO57% (7)
- Biologia de La ConcepcionDocument14 pagesBiologia de La ConcepcionLiss Espana100% (2)
- La AventuraDocument8 pagesLa AventuraDulce Abigail Caamal TunNo ratings yet
- Linfohistiocitosis Hemofagocítica en Pediatría JABMDocument23 pagesLinfohistiocitosis Hemofagocítica en Pediatría JABMJolber Barrantes MedinaNo ratings yet
- Toxoplasmosis: Causas, Síntomas y TratamientoDocument53 pagesToxoplasmosis: Causas, Síntomas y TratamientoJuan Sebastián PinoNo ratings yet
- Ad&d 2.0 - El Desafio Del GuerreroDocument36 pagesAd&d 2.0 - El Desafio Del GuerreroBelle25890No ratings yet
- Reino Protista..Document8 pagesReino Protista..Sandra RenteríaNo ratings yet
- Procesos de La Cría, Recría, Reposición y Engorde de Ganado VacunoDocument46 pagesProcesos de La Cría, Recría, Reposición y Engorde de Ganado Vacunoaponteelera_1967% (6)
- CUESTIONARIO 4 HistologiaDocument5 pagesCUESTIONARIO 4 HistologiaRosangela Macavilca CruzNo ratings yet
- 7º Ensayo de Arnold Ehret: El Diagnóstico Exacto de Tu Enfermedad y "El Espejo Mágico."Document6 pages7º Ensayo de Arnold Ehret: El Diagnóstico Exacto de Tu Enfermedad y "El Espejo Mágico."Charif El Knaichi100% (3)
- Desarrollo Del Aparato DigestivoDocument11 pagesDesarrollo Del Aparato DigestivoFrank Sebastián Domínguez EspínNo ratings yet
- Alteraciones Anomalias DentalesDocument17 pagesAlteraciones Anomalias DentalesxamarraNo ratings yet
- Recetas HamburguesasDocument7 pagesRecetas HamburguesasDescarga100No ratings yet
- Transcripción CATDocument3 pagesTranscripción CATreneeNo ratings yet
- Huesos y MusculosDocument23 pagesHuesos y MusculosSergio CárcamoNo ratings yet
- Enzimas SericasDocument14 pagesEnzimas Sericasmaxsd1977No ratings yet
- Manual Basico para El Cultivo de Peces AmazonicosDocument52 pagesManual Basico para El Cultivo de Peces AmazonicosNicolas Hurtado T.·.No ratings yet
- Guía No. 2. Categorias Gramaticales. Final.Document9 pagesGuía No. 2. Categorias Gramaticales. Final.Diana Natalia Navarrete CastellanosNo ratings yet
- Caso Clinico Leishmania VisceralDocument9 pagesCaso Clinico Leishmania VisceralReinaldo MarinNo ratings yet
- UNIDAD 1 - I - 19 - BlancoDocument52 pagesUNIDAD 1 - I - 19 - BlancoWendy Velasquez RiosNo ratings yet