You might also like
- PID-5-SF 100item Final 2016 PDFDocument9 pagesPID-5-SF 100item Final 2016 PDFRobert PetracheNo ratings yet
- Psychiatric Case PresentationDocument52 pagesPsychiatric Case PresentationdoreenNo ratings yet
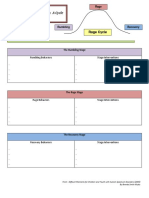
- Rumbling Rage Recovery InfographicDocument4 pagesRumbling Rage Recovery Infographicapi-247044545No ratings yet
- Case Analysis in Psych Bipolar Disorder BYDocument13 pagesCase Analysis in Psych Bipolar Disorder BYSheryl Ann Barit PedinesNo ratings yet
- Mrs. Sunanda's History and Mental Status Exam for DepressionDocument12 pagesMrs. Sunanda's History and Mental Status Exam for DepressionamitNo ratings yet
- Psy Cwu 2Document12 pagesPsy Cwu 2Nadhirah ZulkifliNo ratings yet
- Course Syllabus For Mental Health and Psychiatric NursingDocument2 pagesCourse Syllabus For Mental Health and Psychiatric NursingPhilippineNursingDirectory.com100% (9)
- Erikson's Psychosocial DevelopmentDocument38 pagesErikson's Psychosocial DevelopmentAmeil OrindayNo ratings yet
- HOCDDocument8 pagesHOCDAnonymous R7kU7WNo ratings yet
- Psy Cwu 1Document18 pagesPsy Cwu 1Nadhirah ZulkifliNo ratings yet
- SLE Gordon's Functional Assessment & Physical AssessmentDocument17 pagesSLE Gordon's Functional Assessment & Physical Assessmentjoyrena ochondraNo ratings yet
- Gordon'S 11 Functional Pattern Health Perception-Health Management PatternDocument4 pagesGordon'S 11 Functional Pattern Health Perception-Health Management PatternAnonymous UeEPCPNo ratings yet
- Case ConferenceDocument32 pagesCase ConferenceRuchi TrivediNo ratings yet
- Cases Study On BipolarDocument37 pagesCases Study On BipolarjaoNo ratings yet
- Morning Report 17 SeptemberDocument42 pagesMorning Report 17 SeptemberkadibhaNo ratings yet
- Racket SystemDocument9 pagesRacket Systememilija_milicevic100% (1)
- Sunday, 24 November 2013 Supervisor: DR Sabar P Siregar SP - KJDocument37 pagesSunday, 24 November 2013 Supervisor: DR Sabar P Siregar SP - KJMutiara SazkiaNo ratings yet
- Case Presentation of Bipolar Affective Disorder, Current Episode, Manic With Psychotic DisorderDocument37 pagesCase Presentation of Bipolar Affective Disorder, Current Episode, Manic With Psychotic DisorderEarl John Natividad89% (9)
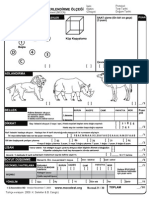
- MOCA Test TurkishDocument1 pageMOCA Test Turkisherkankalem3783No ratings yet
- College of Nursing Ncm101 - Health Assessment DocumentationDocument4 pagesCollege of Nursing Ncm101 - Health Assessment DocumentationAlyssa Marie PepitoNo ratings yet
- Steven Johnsons SyndromeDocument22 pagesSteven Johnsons SyndromeRoselene Mae MarasiganNo ratings yet
- Case Study Acute Pyelonephritis FINALDocument20 pagesCase Study Acute Pyelonephritis FINALRanela Kwinkee Pastor SalazarNo ratings yet
- Patient ReportDocument35 pagesPatient Reportshizaarshad125No ratings yet
- ClinicalDocument61 pagesClinicalokpala ikennaNo ratings yet
- UZAIRDocument11 pagesUZAIRSyed ShahidNo ratings yet
- Case Presentation: - Samraj, Catherine - Thakur, Pratibha - Viswanathan, PreethiDocument107 pagesCase Presentation: - Samraj, Catherine - Thakur, Pratibha - Viswanathan, PreethiRahima AliNo ratings yet
- Palliative Care Group 2C Completed (Final)Document49 pagesPalliative Care Group 2C Completed (Final)Li FaungNo ratings yet
- Case Based Discussion: PsikotikDocument65 pagesCase Based Discussion: PsikotikcorrymarpaungNo ratings yet
- Manic Case ConferenceDocument37 pagesManic Case ConferenceLewis songNo ratings yet
- EXAM BipolarDocument14 pagesEXAM BipolarTiong NeeNo ratings yet
- Mubeena Case FullDocument11 pagesMubeena Case FullSyed ShahidNo ratings yet
- Pramod CaseDocument6 pagesPramod Caselalalalol0021No ratings yet
- Mamta (PDD)Document37 pagesMamta (PDD)RiyaSinghNo ratings yet
- Unspoken Needs KrisnamalDocument26 pagesUnspoken Needs Krisnamalmalaysianhospicecouncil6240No ratings yet
- Schizophrenia Case StudyDocument13 pagesSchizophrenia Case StudysuntharesansivaNo ratings yet
- Morning Report Psychiatric DepartmentDocument51 pagesMorning Report Psychiatric DepartmentaldensmagdalenaNo ratings yet
- Assignment FinalDocument3 pagesAssignment FinalMaukthika ThummalapaaliNo ratings yet
- CBD Case Discussion on a 43-Year-Old Female Patient with Psychotic SymptomsDocument62 pagesCBD Case Discussion on a 43-Year-Old Female Patient with Psychotic SymptomsReza Setyono AshariNo ratings yet
- 'S 11 Functional Health Pattern 1. Health Management PatternDocument7 pages'S 11 Functional Health Pattern 1. Health Management PatternYasminGianneDeOcampoBarizoNo ratings yet
- U. Sayeeda Bano 30 YearDocument11 pagesU. Sayeeda Bano 30 YearSyed ShahidNo ratings yet
- Vivivian PyelonephritisDocument73 pagesVivivian PyelonephritisGideon Owusu AttaNo ratings yet
- SchizophreniaDocument53 pagesSchizophreniaAshishNo ratings yet
- Case Scenario 1 PDFDocument11 pagesCase Scenario 1 PDFMariano MarbellaNo ratings yet
- Morning Report: Friday, 20th March 2015Document37 pagesMorning Report: Friday, 20th March 2015NidaPuspitaAyuNo ratings yet
- Story of A Family - Case Presenation by Mustafa 03-06-2021Document55 pagesStory of A Family - Case Presenation by Mustafa 03-06-2021zNo ratings yet
- Nursing Health HistoryDocument4 pagesNursing Health HistoryhappineselNo ratings yet
- Presentation - PsychiatryDocument21 pagesPresentation - PsychiatrySangkaran KumarNo ratings yet
- Case PresentatiDocument31 pagesCase PresentatiAbdulmajid mohamedNo ratings yet
- Liaison Case Presentation 5: NAJIAH JANJAN (2013489586)Document27 pagesLiaison Case Presentation 5: NAJIAH JANJAN (2013489586)Najiah JanjanNo ratings yet
- Morning Report: Supervisor Dr. Sabar P. Siregar, SP - KJDocument43 pagesMorning Report: Supervisor Dr. Sabar P. Siregar, SP - KJHendra SetyawanNo ratings yet
- Group 3 Presentation.Document37 pagesGroup 3 Presentation.Abdulmajid mohamedNo ratings yet
- Lal Dion Sofi Full CaseDocument9 pagesLal Dion Sofi Full CaseSyed ShahidNo ratings yet
- Marjorie Gordon's Health Pattern: Patients ProfileDocument4 pagesMarjorie Gordon's Health Pattern: Patients ProfileJack BangcoyoNo ratings yet
- Patient with Dengue Fever SyndromeDocument20 pagesPatient with Dengue Fever SyndromeHanako YukaNo ratings yet
- Psychiatric History 1Document6 pagesPsychiatric History 1Stephen Jao Ayala UjanoNo ratings yet
- Group 3 Case Scenario For Status Postpartum With Posttraumatic SyndromeDocument5 pagesGroup 3 Case Scenario For Status Postpartum With Posttraumatic Syndromeaxexrxdxnxaxs zxexlxaxzxnxoxgNo ratings yet
- Clinical Interview for 47-Year-Old Female with Thoracic and Scapular PainDocument5 pagesClinical Interview for 47-Year-Old Female with Thoracic and Scapular PainAsma Mahmood Mahmood AlamNo ratings yet
- Seminar W1 - History Taking in OrthopaedicsDocument23 pagesSeminar W1 - History Taking in OrthopaedicsUN EPNo ratings yet
- Patient'S Profile: MR - Yabi X 64 Years OldDocument5 pagesPatient'S Profile: MR - Yabi X 64 Years OldKrizel Joy TingzonNo ratings yet
- Abdul Basit CASE FULLDocument11 pagesAbdul Basit CASE FULLSyed ShahidNo ratings yet
- Rahul (ATPD)Document34 pagesRahul (ATPD)RiyaSinghNo ratings yet
- Morning Report: Supervisor Dr. Sabar P. Siregar, SP - KJDocument49 pagesMorning Report: Supervisor Dr. Sabar P. Siregar, SP - KJTara WandhitaNo ratings yet
- MSEDocument2 pagesMSEMay Rhezalie PortoNo ratings yet
- Case 7 Bashir AhDocument10 pagesCase 7 Bashir AhSyed ShahidNo ratings yet
- Gordons Kenneth MaternalDocument6 pagesGordons Kenneth Maternalkennedy14344No ratings yet
- OCD Identification and Treatment PlanDocument63 pagesOCD Identification and Treatment PlanHardeep KaurNo ratings yet
- A Radical Behavioral Understanding of The Therapeutic Relationship in Effecting ChangeDocument10 pagesA Radical Behavioral Understanding of The Therapeutic Relationship in Effecting Changejoaomartinelli0% (1)
- Deficient Knowledge CanalesDocument4 pagesDeficient Knowledge CanalesIzhra MargateNo ratings yet
- International Classification of Diseases - 10 Edition: Presentation By-Saloni Punya Akanksha FarheenDocument16 pagesInternational Classification of Diseases - 10 Edition: Presentation By-Saloni Punya Akanksha FarheenAakanksha VermaNo ratings yet
- SandasjkbdjabkdabkajsbdDocument3 pagesSandasjkbdjabkdabkajsbdM Rafif Rasyid FNo ratings yet
- Pyc3701 Chapter 2 - PPTDocument17 pagesPyc3701 Chapter 2 - PPTlauragladwin1No ratings yet
- Maladaptive Exam 1Document20 pagesMaladaptive Exam 1Wen SilverNo ratings yet
- Psychology 2012Document49 pagesPsychology 2012Tom AldertonNo ratings yet
- Globe and MailDocument6 pagesGlobe and MailgregNo ratings yet
- Integrative Behavioral Couple Therapy Vs Traditional Behavioral Couple TherapyDocument8 pagesIntegrative Behavioral Couple Therapy Vs Traditional Behavioral Couple TherapyContención Emocional CIASNo ratings yet
- Conservation of Resources TheoryDocument19 pagesConservation of Resources TheoryYasmine GreenNo ratings yet
- By Sheldon CohenDocument8 pagesBy Sheldon Cohensepta rezitaNo ratings yet
- Understanding Dependent Personality Disorder: Its Causes, Symptoms, and TreatmentDocument15 pagesUnderstanding Dependent Personality Disorder: Its Causes, Symptoms, and TreatmentEvren ManaguitNo ratings yet
- What Spying On Your Loved Ones Can Lead ToDocument1 pageWhat Spying On Your Loved Ones Can Lead ToMaria StephanieNo ratings yet
- Aspire Issue 6Document41 pagesAspire Issue 6HelenNo ratings yet
- Autism and SnoezelenDocument2 pagesAutism and SnoezelenTeona MelinteNo ratings yet
- Research into Coma, Esdaile and Sichort States offers New InsightsDocument10 pagesResearch into Coma, Esdaile and Sichort States offers New Insightscoach rismanNo ratings yet
- Elc 590 - English For Oral Presentations Informative SpeechDocument6 pagesElc 590 - English For Oral Presentations Informative SpeecherynnaeimmanNo ratings yet
- Modern Media Vs Self-EsteemDocument8 pagesModern Media Vs Self-Esteemapi-460400351No ratings yet
- Unit 2: Aspects of Personal DevelopmentDocument32 pagesUnit 2: Aspects of Personal DevelopmentDaniella May Calleja0% (1)
- Investigation Report 2Document13 pagesInvestigation Report 2Riley MurdockNo ratings yet
- Chapter 3Document3 pagesChapter 3Black PantherNo ratings yet
- Technology in CounsellingDocument18 pagesTechnology in CounsellingWilly TanNo ratings yet
- Profiles Best Revised Matrix 2010Document2 pagesProfiles Best Revised Matrix 2010api-235377542No ratings yet