You might also like
- Assessment and Evaluation: 2008 Edition Rhoda K Hahn, MD Lawrence J. Albers, MDDocument85 pagesAssessment and Evaluation: 2008 Edition Rhoda K Hahn, MD Lawrence J. Albers, MDAlbghdadi CristianNo ratings yet
- Clerkship - Psychiatric History and MseDocument24 pagesClerkship - Psychiatric History and MsefahmiNo ratings yet
- Prescribing Psychotropics: From Drug Interactions to PharmacogeneticsFrom EverandPrescribing Psychotropics: From Drug Interactions to PharmacogeneticsRating: 5 out of 5 stars5/5 (1)
- PMHNP Case Study - EditedDocument7 pagesPMHNP Case Study - EditedSoumyadeep BoseNo ratings yet
- Psychiatry Practice Boosters 2016: Insights from research to enhance your clinical workFrom EverandPsychiatry Practice Boosters 2016: Insights from research to enhance your clinical workNo ratings yet
- High Yield PsychiatryDocument43 pagesHigh Yield Psychiatryconfusedmage91% (11)
- Psychiatry High Yield NotesDocument6 pagesPsychiatry High Yield Notesgregry2100% (2)
- Psychiatry Practice Boosters, Second Edition: Insights from research to enhance your clinical workFrom EverandPsychiatry Practice Boosters, Second Edition: Insights from research to enhance your clinical workNo ratings yet
- Psych TemplateDocument1 pagePsych TemplateWilliam Yang100% (1)
- SCTL NeurotransmitterDocument32 pagesSCTL Neurotransmitternur qistina humaira zulkarshamsiNo ratings yet
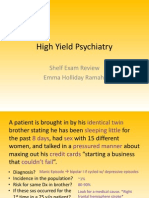
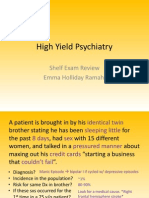
- High Yield Psychiatry: Shelf Exam Review Emma Holliday RamahiDocument43 pagesHigh Yield Psychiatry: Shelf Exam Review Emma Holliday Ramahigreg100% (1)
- 2012-13 Psychiatry Board ReviewDocument79 pages2012-13 Psychiatry Board Reviewlizzy596100% (1)
- Cases from the Psychiatry Letter - I: Cases from the Psychiatry Letter, #1From EverandCases from the Psychiatry Letter - I: Cases from the Psychiatry Letter, #1Rating: 5 out of 5 stars5/5 (1)
- Psychiatry Shelf ReviewDocument11 pagesPsychiatry Shelf ReviewAhmad Syahmi YZ75% (4)
- Psychiatry Made Simple: Dr. Pete’S Guide to Your Mental HealthFrom EverandPsychiatry Made Simple: Dr. Pete’S Guide to Your Mental HealthNo ratings yet
- Psychiatry - Shelf ReviewDocument101 pagesPsychiatry - Shelf Reviewluck2liv100% (4)
- SPMM 2015 FullDocument1,610 pagesSPMM 2015 FullAnamika Sinha100% (4)
- Descriptive Psychopathology (Synopsis of Symptoms of The Mind)Document35 pagesDescriptive Psychopathology (Synopsis of Symptoms of The Mind)hungryscribeNo ratings yet
- Study Guide For The Psychiatry NBME Content Exam AKA The Psychiatry Shelf Exam!Document2 pagesStudy Guide For The Psychiatry NBME Content Exam AKA The Psychiatry Shelf Exam!DoriNo ratings yet
- K P Differential Diagnosis Pyramid: OPMAPS: Sychiatry EvisionDocument36 pagesK P Differential Diagnosis Pyramid: OPMAPS: Sychiatry EvisionArama CristiNo ratings yet
- DSM-IV Criteria MnemonicsDocument4 pagesDSM-IV Criteria Mnemonicsleonyap100% (1)
- Structured Approach To Acute Psychiatry EmergenciesDocument41 pagesStructured Approach To Acute Psychiatry EmergenciesRaimondo RomanazziNo ratings yet
- Psychiatric History - MSEDocument7 pagesPsychiatric History - MSEDeepbluex100% (1)
- Psychiatry Notes & Suicide Risk Assessment Templates - USMLE Step 2CKDocument33 pagesPsychiatry Notes & Suicide Risk Assessment Templates - USMLE Step 2CKDuncan89100% (1)
- Psych Menmonics (Random)Document22 pagesPsych Menmonics (Random)Kaly RieNo ratings yet
- Varun Kumar, 2017 - Getting Started in PsychiatryDocument148 pagesVarun Kumar, 2017 - Getting Started in PsychiatryBernard FZ100% (1)
- Psychiatry Study Guide For ShelfDocument42 pagesPsychiatry Study Guide For Shelfappolinia64% (14)
- HighYieldPsychiatry PDFDocument43 pagesHighYieldPsychiatry PDFYay100% (4)
- 72 PerinatalPsychiatry PDFDocument11 pages72 PerinatalPsychiatry PDFCetVital100% (1)
- Psychiatric Clinical SkillsDocument376 pagesPsychiatric Clinical SkillsSamuel Agunbiade100% (5)
- Psychiatry MnemonicsDocument4 pagesPsychiatry MnemonicsHiruni Tharuka100% (2)
- First Rank Symptoms of SchizophreniaDocument65 pagesFirst Rank Symptoms of Schizophreniadrkadiyala2No ratings yet
- Psychiatry Beginners ManualDocument132 pagesPsychiatry Beginners ManualGabriel Viana SilveiraNo ratings yet
- KAPLAN Study Guide Ninth Edition-1 (001-100) PDFDocument100 pagesKAPLAN Study Guide Ninth Edition-1 (001-100) PDFflorNo ratings yet
- Week 2 (OSCE CASC Book II 2018-19) 03.09.2018Document48 pagesWeek 2 (OSCE CASC Book II 2018-19) 03.09.2018Andrew WdsmithNo ratings yet
- 7718 (07) Review of Cases - Anxiety DisordersDocument34 pages7718 (07) Review of Cases - Anxiety Disordersnewaz100% (1)
- Introduction To Psychiatric Interviewing: Page 1 of 6Document6 pagesIntroduction To Psychiatric Interviewing: Page 1 of 6Bruno BatinicaNo ratings yet
- Resident's Guide To Clinical PsychiatryDocument412 pagesResident's Guide To Clinical PsychiatryJP Rajendran88% (16)
- Blueprints PsychiatryDocument466 pagesBlueprints Psychiatrynoir100% (5)
- Psychiatry Shelf Spreadsheet P.montenigro M3Document5 pagesPsychiatry Shelf Spreadsheet P.montenigro M3JamesHowson100% (1)
- GMT 409 Psychiatry Student Guide BookDocument43 pagesGMT 409 Psychiatry Student Guide BookAhmad Syahmi YZ100% (1)
- Current Clinical Strategies Psychiatry - Rhoda K HahnDocument125 pagesCurrent Clinical Strategies Psychiatry - Rhoda K HahnLetitia Claudia DobraniciNo ratings yet
- Psychiatry PDFDocument31 pagesPsychiatry PDFDeepNo ratings yet
- Notes PsychiatryDocument36 pagesNotes Psychiatryvinodksahu0% (1)
- PsychiatryDocument95 pagesPsychiatryJarwoto RoestanajieNo ratings yet
- Quick Reference Guide April 2019 PDFDocument2 pagesQuick Reference Guide April 2019 PDFAaron ShokarNo ratings yet
- Review Notes 2000 - PsychiatryDocument56 pagesReview Notes 2000 - Psychiatryeset5No ratings yet
- Simple CASC StationsDocument74 pagesSimple CASC Stationssherief marouf100% (2)
- Case History, MSE and Rating Scales - in Psychological AssessmentDocument29 pagesCase History, MSE and Rating Scales - in Psychological Assessmentsu84No ratings yet
- Psychopathology Signs and Symptoms in Psychiatry: Third Edition Patricia CaseyDocument35 pagesPsychopathology Signs and Symptoms in Psychiatry: Third Edition Patricia CaseyValsala Baskaran100% (3)
- Dementia: Diagnosis and TreatmentDocument53 pagesDementia: Diagnosis and Treatmentakashdeep050% (1)
- The Ninja'S Guide To Prite: 2019 Question BookDocument181 pagesThe Ninja'S Guide To Prite: 2019 Question BooknonsNo ratings yet
- Clinical Methods in Psychiatry 2nd EditionDocument92 pagesClinical Methods in Psychiatry 2nd Editionprachirb100% (1)
- Psychiatry CasesDocument65 pagesPsychiatry CasesakeelNo ratings yet
- Antipsychotics: Crash Course Lecture July 2016 VersionDocument101 pagesAntipsychotics: Crash Course Lecture July 2016 Versionyepherenow100% (1)
- Step 3 Sample Questions 2015Document41 pagesStep 3 Sample Questions 2015yepherenow100% (2)
- DX of Aom or OmeDocument1 pageDX of Aom or OmeyepherenowNo ratings yet
- Visual Mnemonics For BoardsDocument39 pagesVisual Mnemonics For BoardsyepherenowNo ratings yet
- Brochure DRX Revolution 201507Document8 pagesBrochure DRX Revolution 201507غزوان عماد الدين الحسينيNo ratings yet
- Cardiology Summary PDFDocument62 pagesCardiology Summary PDFSyamsuriWahyuNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakahaseosamaNo ratings yet
- Journal of Clinical and Medical ImagesDocument3 pagesJournal of Clinical and Medical Imagesliterature publishersNo ratings yet
- Ob 1.05 Clinical Practice Guidelines On Immunization For Filipino WomenDocument7 pagesOb 1.05 Clinical Practice Guidelines On Immunization For Filipino Womenotartil_niman50% (2)
- 3 Days Implant Course - PDF FinalDocument6 pages3 Days Implant Course - PDF FinalShivamNo ratings yet
- PBR Announcement Final PostingDocument7 pagesPBR Announcement Final PostingLoki PagcorNo ratings yet
- Pedia2 Sepsis (Dr. Seng)Document3 pagesPedia2 Sepsis (Dr. Seng)Tony DawaNo ratings yet
- Hydroxychloroquine SulfateDocument20 pagesHydroxychloroquine Sulfategiamatti2005No ratings yet
- The Brooklyn Cancer Center Announces New Chief of Hematology-OncologyDocument3 pagesThe Brooklyn Cancer Center Announces New Chief of Hematology-OncologyPR.comNo ratings yet
- List of Abbreviations Used in Medical PrescriptionsDocument25 pagesList of Abbreviations Used in Medical PrescriptionsDiana MuañaNo ratings yet
- Anatomy of The Lingual Vestibule and Its Influence On Denture Borders 2161 0940.1000122Document4 pagesAnatomy of The Lingual Vestibule and Its Influence On Denture Borders 2161 0940.1000122Purnama SyahbaniNo ratings yet
- Netherlands Academic Medical Center University of AmsterdamDocument2 pagesNetherlands Academic Medical Center University of AmsterdamCristianpalmarNo ratings yet
- Detecting Autism Early - A Pilot To Train Providers, Screen Toddlers, and Support Families With Autism Concerns in Primary CareDocument41 pagesDetecting Autism Early - A Pilot To Train Providers, Screen Toddlers, and Support Families With Autism Concerns in Primary CareAUCDNo ratings yet
- Dr. SumariyonoDocument1 pageDr. SumariyonoYosuaNo ratings yet
- Course Outline PHC 2019Document3 pagesCourse Outline PHC 2019Teslim RajiNo ratings yet
- Classification For Zygomatic Implant PatientsDocument7 pagesClassification For Zygomatic Implant PatientsDrVarun Menon50% (2)
- Materi - Departments in The Hospital and Giving Direction-Merged-DikonversiDocument12 pagesMateri - Departments in The Hospital and Giving Direction-Merged-DikonversiAch Fani FerdianNo ratings yet
- Neuro-Oncology Training For The Child Neurology ResidentDocument7 pagesNeuro-Oncology Training For The Child Neurology ResidentMaurycy RakowskiNo ratings yet
- Gingival and PeriodontalDocument57 pagesGingival and PeriodontalPhanQuangHuyNo ratings yet
- L.orpilla Jomark C. LFDDocument2 pagesL.orpilla Jomark C. LFDmark OrpillaNo ratings yet
- QRST CV!!!Document4 pagesQRST CV!!!Menaliza TomasNo ratings yet
- Standardization of Sitopaladi Churna: A Poly-Herbal FormulationDocument12 pagesStandardization of Sitopaladi Churna: A Poly-Herbal Formulationdrsa2No ratings yet
- Pediatric BurnsDocument19 pagesPediatric BurnsmalindaNo ratings yet
- Service Blue PrintDocument3 pagesService Blue Printtinornit0% (1)
- Osteochondroma Is The Most Common Benign Bone TumorDocument20 pagesOsteochondroma Is The Most Common Benign Bone TumorMo LiraNo ratings yet
- Idiopathic Thrombocytopenic Purpura: Bruising Petechiae Nosebleeds GumsDocument7 pagesIdiopathic Thrombocytopenic Purpura: Bruising Petechiae Nosebleeds GumsMahirina Marjani ZulkifliNo ratings yet
- Kim 2012Document9 pagesKim 2012zaheerbdsNo ratings yet
- Stryker VariAx Foot Locking Plate System PDFDocument28 pagesStryker VariAx Foot Locking Plate System PDFJacob DoughertyNo ratings yet
- CBCT-Scan in DentistryDocument24 pagesCBCT-Scan in DentistryBilly Sam80% (5)